Impact of Diagnosis-Based Payment Reform on China's Healthcare Industry
On January 16, the National Development and Reform Commission (NDRC), in conjunction with the National Health and Family Planning Commission (NHFPC) and the Ministry of Human Resources and Social Security (MOHRSS), jointly issued the “Notice on Promoting Diagnosis-Related Group (DRG) Payment Reform,” deciding to further deepen pilot programs on the basis of existing initiatives by implementing diagnosis-based payment for 320 specified medical conditions. The Notice also clearly outlined the implementation timeline.
Advancing Diagnosis-Related Group (DRG) Payment: Expanding Scope and Tightening Regulations
Diagnosis-Related Group (DRG) payment is a prospective reimbursement model for health insurance that is widely adopted internationally. Countries such as the United States, Germany, Australia, Japan, and South Korea have all incorporated this model into their health insurance payment systems to varying degrees. Unlike the common practice in China, where patients receive medical consultations first and payments are made based on actual medical services rendered, the prospective payment system determines the reimbursement amount before the patient receives medical services. Consequently, healthcare providers bear greater financial risk and are incentivized to proactively control costs and reduce expenditures.
The core of diagnosis-related group (DRG) pricing is to classify and price medical services based on disease types, severity levels, and other factors, with health insurance funds reimbursing hospitals according to these predetermined rates. The National Development and Reform Commission’s recent issuance of another policy document to advance DRG-based payment pilots clearly aims to control overall healthcare expenditures and alleviate the financial burden on both patients and the health insurance system.
China’s first national-level exploration of case-based payment began in 2004 with the issuance of the “Notice on Launching Pilot Programs for Case-Based Payment Management” by the General Office of the Ministry of Health, initiating pilots in provinces and municipalities including Heilongjiang, Liaoning, Tianjin, Shandong, Shaanxi, Henan, and Qinghai. During the pilot phase, the main challenges encountered were low participation and lack of coordination among health insurance payers, coupled with insufficient hospital informatization and standardization, which hindered the widespread adoption of diagnosis-based accounting and payment methods.
In January 2017, the “Notice on Promoting Diagnosis-Related Group (DRG) Payment” required that pilot regions for comprehensive reform of public hospitals in urban areas implement DRG-based payment for no fewer than 100 disease categories by the end of 2017. Compared with previous policies, this Notice features an expanded scope and stricter regulations.
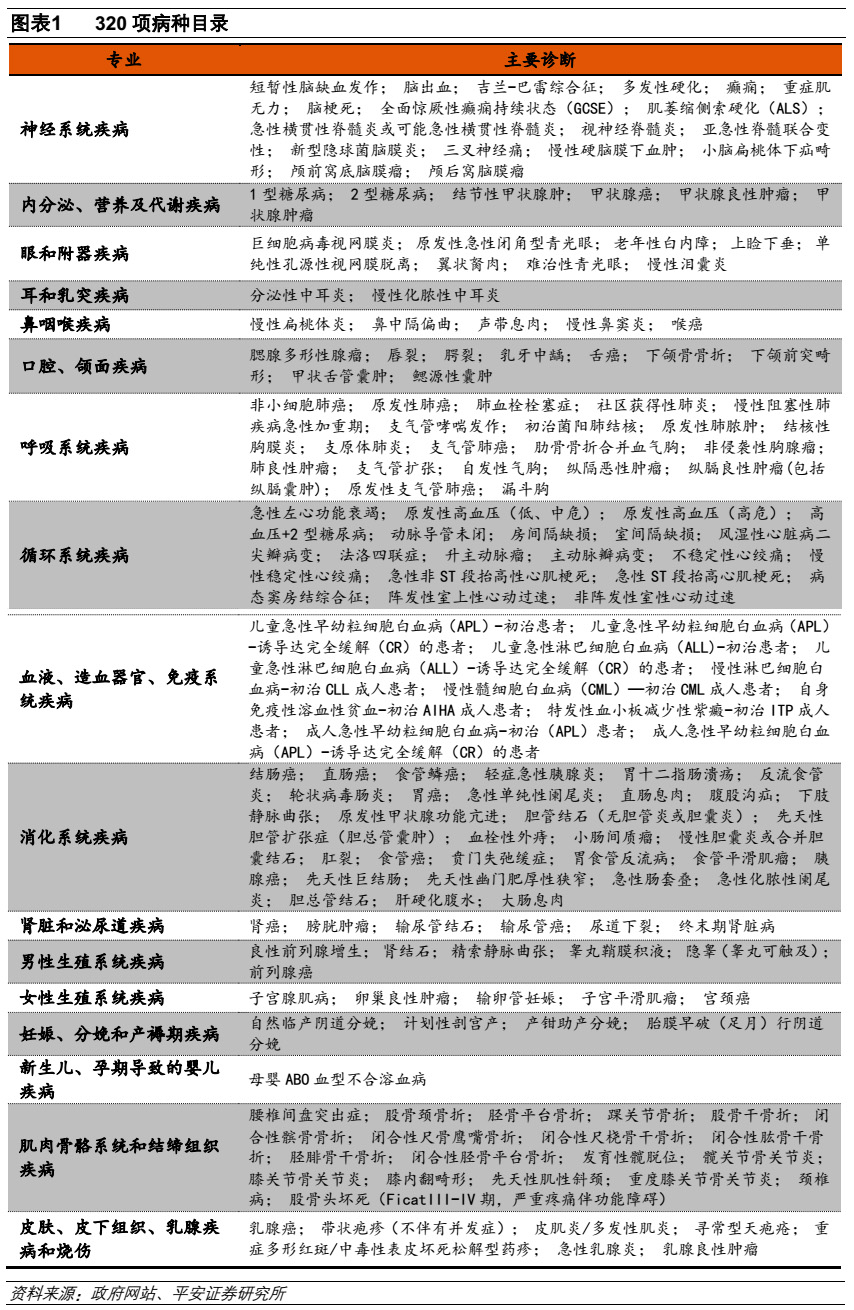
In terms of scope, the "Notice" requires all regions to further expand the number of diseases covered under case-based payment, building upon earlier pilot reforms. In 2011, the list of diseases included in the pilot comprised over one hundred conditions; individual hospitals typically selected 30–100 of these for case-based payment implementation, depending on their size and classification. The current document expands the pilot disease list to 320 items, covering 17 relatively independent disease categories with low complication rates, including those affecting the nervous system, metabolism, sensory organs (ear, nose, throat, and eyes), respiratory system, blood system, and immune system. Furthermore, it mandates that by the end of 2017, each pilot hospital must implement payment reform for no fewer than 100 disease types, representing a significant increase compared to previous requirements.
From a regulatory perspective, the 2017 version of the “Notice” refined and standardized certain implementation details, thereby reducing the potential for deviations during execution. For instance, it specifically clarified the definition of fees. It stipulates that diagnosis-related group (DRG)-based pricing for medical services refers to the practice whereby medical institutions charge patients using specific disease categories as the unit of pricing. The fee schedule covers all expenses incurred from admission for diagnosis to discharge following standardized treatment for the specified condition, including costs for diagnosis, treatment, surgery, anesthesia, nursing care, bed charges, pharmaceuticals, and medical consumables. In principle, hospitals are prohibited from imposing additional charges beyond the established DRG-based fee standards. Furthermore, examination and testing costs incurred after admission must not be reclassified as outpatient charges. Essentially, this encompasses all medical expenditures, with the exception of bed charges that exceed the standards covered by medical insurance.
Furthermore, the "Notice" requires medical institutions not to refuse critically ill patients, not to unjustifiably shorten hospital stays, and not to split single hospitalizations into multiple admissions. It also proposes incorporating diagnosis-related group (DRG) payment into the performance evaluation system for public medical institutions to ensure that these institutions have sufficient incentive and initiative to implement the document.
As required by the documents, local supporting regulations are expected to be implemented by the end of June 2017. Currently, issues such as how medical insurance will be integrated, how clinical pathways will be confirmed, and how physicians’ interests will be safeguarded remain unclear; these matters are expected to be clarified within six months.
Model Transformation Drives Industry Change
Although there are still many uncertainties surrounding the current implementation of diagnosis-related group (DRG) payment policies, it is certain that, overall, DRG-based reimbursement will inevitably reduce medical costs for relevant diseases, exerting certain pricing pressure on manufacturers across various sub-sectors. Specifically, the characteristics of industry changes will include the following three points:
Currently, pharmaceutical revenue still accounts for a significant proportion of hospital income; however, in terms of the impact brought by diagnosis-related group (DRG) payment reform, we believe that medical devices are likely to be more significantly affected.
On one hand, the policy of eliminating drug markups has been intensively implemented in many regions, weakening the link between pharmaceuticals and hospital profitability. In contrast, medical devices, equipment, and consumables—whether high-value items such as implants or reagents and supplies used for diagnostic testing—remain significant sources of revenue for hospitals to date. Once diagnosis-related group (DRG) payment is adopted, these devices and consumables will shift directly from revenue items to cost items, substantially increasing hospitals’ incentive to drive down prices.
On the other hand, although documents issued by certain provinces and municipalities prohibit hospitals from directing patients to purchase medications outside the hospital, regulatory enforcement remains challenging. Given the current presence of in-hospital pharmacies and adjacent retail pharmacies, we believe that following the implementation of diagnosis-related group (DRG) payment systems, a scenario may arise where high-priced drugs are not provided by hospitals, necessitating out-of-hospital purchases. However, as most medical devices and consumables have highly specialized application scenarios and lack a reasonable rationale for retail pharmacy distribution, we consider the management of their usage to be relatively easier.
After years of development, the quality of domestically produced pharmaceutical products in China has improved significantly compared to the past. The government is encouraging domestic products to replace imports through measures such as the consistency evaluation of generic drugs, promoting the research and development of biosimilars, and selecting outstanding domestically made medical equipment. However, imported products, especially high-end devices, still hold a large market share in major hospitals. There are many reasons behind this, but an important one is that the absolute prices of imported products are high, and a considerable number of provinces and cities set higher service fees when using imported equipment for medical services, giving hospitals an incentive to use imported products. Once payment by disease type is implemented, the lower prices of domestic products will be highly attractive to hospitals.
Taking chemiluminescent hepatitis B two-and-a-half pairs testing as an example, the cost of imported reagents is around 50 yuan, while that of domestically produced reagents is 20 yuan. When the test can no longer be billed separately, the standalone pricing advantage of imported products disappears; in contrast, adopting domestically produced reagents will help hospitals save 30 yuan in costs.
In recent years, many enterprises have joined the wave of building third-party service platforms; however, the overall scale remains limited to date. The primary reason is that the establishment of such platforms undermines hospitals’ financial interests, leaving them with little incentive to outsource these revenue-generating services. Most successfully operated third-party centers have primarily relied on differentiated operational strategies to avoid direct conflicts of interest with hospitals. Under diagnosis-related group (DRG) payment systems, departments such as medical imaging, clinical laboratory, and pathology no longer serve as revenue generators but instead become cost items deducted from insurance payments. Nevertheless, diagnostic services like imaging and laboratory testing remain indispensable components of healthcare. Therefore, we believe that the scalable advantages of third-party centers are poised to be fully realized.
On the other hand, although the centralized supply model keeps these departments’ operations within the hospital, its core advantages—leveraging volume for price concessions and providing ancillary services—can help hospitals reduce costs through alternative means. This achieves effects similar to those of third-party platforms, making it a viable operational model in a diagnosis-related group (DRG)-based payment environment.
Report Source: Ping An Securities