Investment Opportunities in Grassroots Healthcare in 2017 (Part I): Which Industries Benefit from the Rise of Primary Care Services?
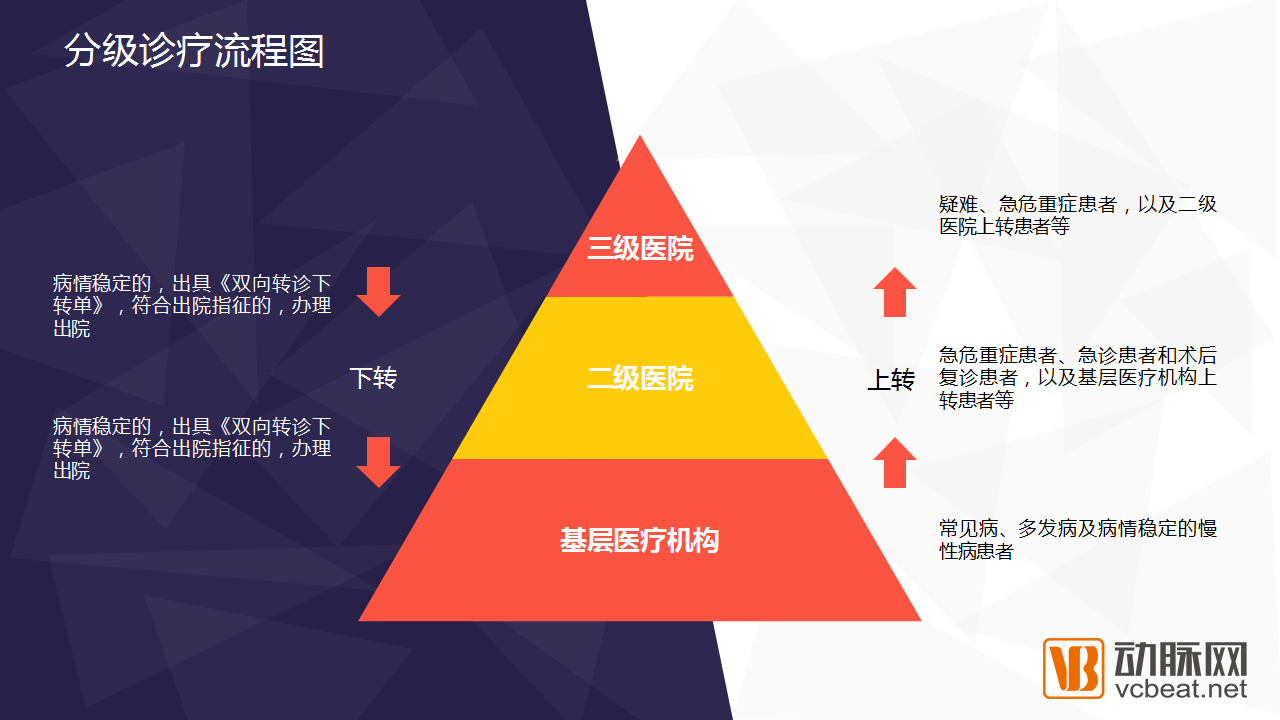
Implementing tiered diagnosis and treatment has been the top priority of China’s new healthcare reform. By optimizing the allocation of medical resources, hospitals at different levels can establish effective division of labor and collaboration, thereby alleviating the current shortage in medical service supply. In simpler terms, this means classifying diseases based on their severity and urgency, assigning treatment responsibilities to medical institutions of corresponding levels, and thus easing the difficulty residents face in accessing medical care.
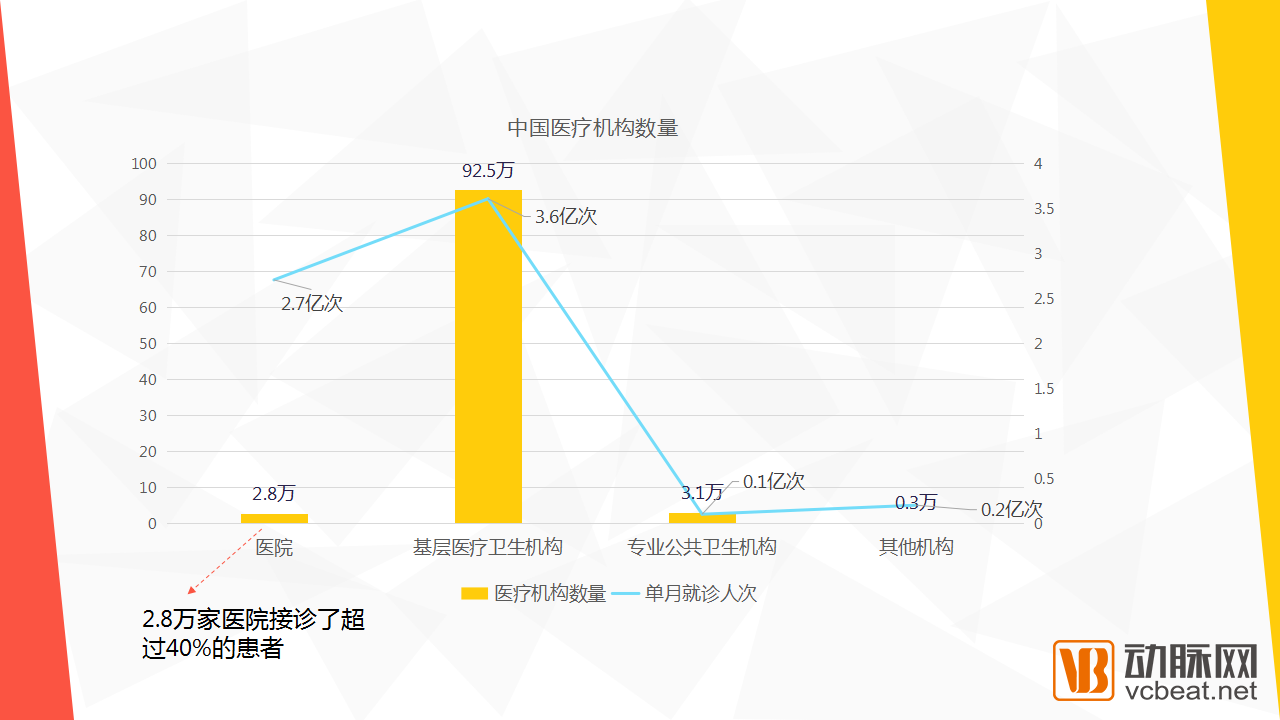
As of the end of April 2016, the number of medical and health institutions across China reached 988,000, including: 28,000 hospitals, 925,000 primary healthcare institutions, 31,000 specialized public health institutions, and 3,000 other medical institutions. Primary healthcare institutions account for an overwhelmingly high proportion in terms of quantity within China’s healthcare service system, reaching 93.6%. However, their share of clinical visits is far lower than their proportional representation by numbers. Taking April 2016 as an example, primary healthcare institutions handled only 54.5% of total outpatient visits, while hospitals accounted for 40.9%. This means that less than 3% of all medical institutions—namely hospitals—attended to 40.9% of patients. The concentration of patients seeking care at large hospitals has exacerbated difficulties in accessing medical services, making the implementation of a tiered diagnosis and treatment model imperative.
In the preceding section, we analyzed the patient volume handled by medical institutions at various levels, highlighting the differences in the number of patient visits. In terms of total healthcare revenue, hospital inpatient services, hospital outpatient services, and primary care services account for approximately 60%, 25%, and 15%, respectively, of national healthcare expenditure. The goal of tiered diagnosis and treatment is to redirect hospital outpatient visits to primary care institutions. Therefore, from a trend perspective, the share of hospital inpatient services is not expected to change significantly in the future, while a substantial portion of hospital outpatient services will shift to the primary care level. Revenue from primary care services is projected to rise continuously to around 20%, reaching parity with or even surpassing that of hospital outpatient services. In terms of the proportion of clinical encounters, the total number of patient visits to primary care institutions is expected to increase substantially from the current 54.5% to 70%.
Since 2016, the Chinese government has introduced numerous policies to accelerate the implementation of a tiered diagnosis and treatment system. In January 2017, multiple additional policies related to this system were rolled out in quick succession, which are expected to drive growth in industries associated with primary healthcare and significantly enhance investment opportunities in this sector.
In January 2017, the National Conference on Medical Administration made specific arrangements for medical administration work in 2017. The five key priorities for 2017 were: First, advance the development of a tiered diagnosis and treatment system to establish an orderly healthcare-seeking pattern. Second, continue implementing the Action Plan for Improving Medical Services and optimize the allocation of medical resources to enhance the public’s sense of gain in health. Third, deepen targeted health-focused poverty alleviation efforts to support the campaign against poverty. Fourth, safeguard medical quality and safety, adhering strictly to the baseline standards of service. Fifth, comprehensively strengthen Party building and professional conduct, fostering integrity and a positive ethos within the industry.
In January 2017, the State Council issued the “13th Five-Year Plan for Deepening the Reform of the Medical and Healthcare System.” During the 13th Five-Year Plan period, China will achieve new breakthroughs in the development of five key systems: tiered diagnosis and treatment, modern hospital management, universal health insurance, drug supply guarantee, and comprehensive regulation. The Plan places tiered diagnosis and treatment at the forefront of the reforms, with the family doctor contract system serving as a crucial driver for its implementation.
In January 2017, the National Health and Family Planning Commission convened the 2017 National Conference on Primary Healthcare in Beijing, advancing primary healthcare work according to a “two verticals and three horizontals” roadmap. The “two verticals” refer to strengthening the construction of rural and urban primary healthcare service networks, while the “three horizontals” focus on effectively addressing key issues in basic public health services in urban and rural areas, workforce shortages, and the guiding and supportive role of medical insurance.
In June 2016, seven national ministries and commissions jointly issued the “Guiding Opinions on Promoting Family Doctor Contract Services.” The targets set forth in the “Opinions” were to achieve a family doctor contract service coverage rate of over 30% by 2017, with a coverage rate of over 60% for key populations. By 2020, efforts would be made to expand contract services to the entire population, establish long-term and stable contractual service relationships, and basically achieve full coverage of the family doctor contract service system.
In April 2016, Premier Li Keqiang presided over an executive meeting of the State Council to determine the key priorities for deepening healthcare system reform in 2016. The measures included accelerating the training of general practitioners and pediatricians, launching pilot programs for tiered diagnosis and treatment in approximately 70% of prefecture-level cities nationwide, initiating pilots allowing attending physicians and above from public hospitals (either incumbent or retired) to practice or establish studios at primary care institutions, and ensuring that family doctor contract services covered more than 15% of the population by the end of the year.
In September 2015, the General Office of the State Council issued the “Guiding Opinions on Advancing the Construction of a Tiered Diagnosis and Treatment System,” clearly stating that by 2017, the policy framework for tiered diagnosis and treatment would be progressively improved, a basic mechanism for division of labor and collaboration among medical and health institutions would be established, high-quality medical resources would be systematically and effectively decentralized to lower levels, and the development of primary healthcare workforce—with general practitioners as the focus—would be strengthened. It proposed that pilot regions for tiered diagnosis and treatment should meet several operational standards, including a compliance rate of ≥95% for the construction of primary medical and health institutions, and primary care visits accounting for ≥65% of total medical consultations, among others.
During the development of internet-based healthcare, one policy proved particularly significant: the “Opinions on Implementing Appointment-Based Diagnosis and Treatment Services in Public Hospitals,” issued by the Ministry of Health in 2009. The emergence of internet technology made informatization a key means of optimizing medical processes. It was precisely the release of this document that launched the industrial journey of internet healthcare, endorsing the concept of “centralized appointment-based diagnosis and treatment platforms.” This enabled companies whose core business revolved around online registration—such as WeDoctor (Guahao.com) and Jiuyi160—to achieve rapid growth.
In the implementation of the tiered diagnosis and treatment policy, the state began promoting family doctor contract services in mid-2016, aiming to achieve a family doctor service coverage rate of over 30% and a contract service coverage rate for key populations of over 60% by 2017. The policy established specific evaluation criteria to be met by the end of 2017. Meeting these standards will bring about disruptive changes to China’s medical environment and care models, while also creating new investment opportunities for the internet healthcare industry. In addition to administrative measures driving tiered diagnosis and treatment, economic incentives are also being employed, with many regions having relaxed licensing restrictions for private medical institutions. Primary care and community medical institutions suffer from outdated equipment and lower levels of physician expertise; these deficiencies represent significant business opportunities. Supported by policy, the RMB 450 billion primary care market is opening up to private entities. Although primary care constitutes only the foundational layer of healthcare reform, it is undoubtedly the segment with the largest volume and the most urgent demand. Under these circumstances, those who possess more primary care resources will be better positioned to break through and succeed.
VCBeat has published numerous articles analyzing the changes that tiered diagnosis and treatment and family doctor services bring to both doctors and patients, so there is no need to elaborate on this here. Instead, we will focus on analyzing which industries will directly benefit from the promotion of tiered diagnosis and treatment, as well as the new investment opportunities it will generate.
Healthcare IT enterprises will reap substantial benefits from the advancement of tiered diagnosis and treatment.
HIS Cloud for Primary Healthcare Institutions
In the tiered diagnosis and treatment system, the upward and downward referral of patients among primary healthcare institutions, county-level hospitals, and higher-level medical institutions is a critical issue. Therefore, there is an urgent need to achieve interoperability of information across these institutional levels. Primary healthcare institutions suffer from low levels of informatization, resulting in substantial demand for information technology infrastructure development.
Insufficient funding for primary healthcare institutions is a bottleneck restricting the development of health informatics. Cloud-based HIS, leveraging cloud services, offers greater cost advantages over traditional HIS for primary healthcare institutions and is thus more readily adopted. Furthermore, Cloud-based HIS is easier to maintain in later stages compared to traditional HIS systems, virtually eliminating the need to establish specialized maintenance teams and thereby reducing IT expenditures for healthcare institutions.
Under the tiered diagnosis and treatment policy, medical consortia and physician groups serve as key pathways for its implementation. Given the substantial investment and lengthy construction periods associated with Hospital Information Systems (HIS) in tertiary hospitals, the likelihood of completely overhauling these systems is extremely low. Meanwhile, cloud-based HIS solutions adopted by primary healthcare institutions must ensure compatibility with those used by higher-level institutions to achieve seamless information interoperability. Consequently, established healthcare IT companies hold a competitive advantage in promoting their products within primary healthcare settings.
Doctor Tools: Patient Management
A key component of the tiered diagnosis and treatment system is the family doctor service contract scheme. In line with the 2017 target of achieving a family doctor service coverage rate of over 30%, each family doctor is responsible for the health management of more than a thousand residents, particularly high-risk populations suffering primarily from chronic diseases such as hypertension, diabetes, and tuberculosis. Effective management of community patient records and enhanced doctor-patient communication will create new market growth opportunities for IT solution providers serving physicians.
In traditional hospitals, the hospital information system facilitates the efficient management and retrieval of patient medical records, medical imaging, laboratory reports, and prescriptions. However, family doctors in primary healthcare institutions operate in a different environment, often requiring home visits to residents. Therefore, it is crucial to enable the retrieval and entry of patients’ historical data via mobile terminal devices, allowing for on-the-go data query and input.
Physician Tools: Clinical Decision Support
Tiered diagnosis and treatment impose higher demands on physicians in primary healthcare institutions, with general practitioners representing the largest shortage among China’s current medical workforce. Furthermore, due to historical reasons, general practitioners lack sufficient clinical experience.
For physicians, acquiring specialized medical knowledge is crucial; however, the vast array of medical terminology, disease classifications, medication dosages, and contraindications within the healthcare system cannot be fully mastered by every doctor, particularly general practitioners. Electronic clinical decision support tools can provide primary care general practitioners with comprehensive professional knowledge and information across all areas of general practice, along with various medication-based calculation and assessment tools, thereby offering decision support to enhance their diagnostic and therapeutic services.
Physician Training
There is extreme polarization in the competency of physicians in China, with hospital tier levels essentially serving as a proxy for clinical expertise. Physicians at primary care institutions are eager to excel and have never slackened their efforts to acquire medical knowledge and skills. However, due to a lack of learning opportunities and resources, their professional competence has long remained stagnant. Standardized residency training for primary care physicians at tertiary hospitals often becomes a mere formality, as these host institutions frequently fail to dedicate sufficient effort or resources to their training.
Telemedicine System
Since the launch of internet-based healthcare in China, the demand for telemedicine systems in primary healthcare institutions is expected to increase significantly. Even township health centers with modest facilities can receive technical guidance from specialists, and patients can benefit from remote consultations with experts, thereby sparing them the hardship of long-distance travel.
In large cities, family doctors and community healthcare institutions are deeply embedded within communities, enabling residents to access upward referrals with ease. In addition to consultation systems, health data collection and monitoring platforms, as well as medical emergency call systems for residents, can be introduced. When a resident experiences an acute medical emergency, family doctors can provide on-site management and first aid more rapidly than the 120 emergency medical services, delivering critical care during the “golden six minutes” of emergency treatment to save patients’ lives.
In the field of IVD (in vitro diagnostics), point-of-care testing(POCT)The product is poised to capture significant market share. With their compact and portable design, ease of use, and rapid turnaround time for results, point-of-care diagnostic products are well-suited for primary healthcare services.
POCT
POCT is a branch of the in vitro diagnostics (IVD) field. The POCT product market is primarily concentrated in four categories: blood glucose meters, pregnancy tests, blood gas and electrolyte analyzers, and disease marker testing. POCT products include portable analytical instruments and their corresponding reagents, featuring portability, ease of operation, and immediate reporting. These characteristics make them highly suitable for primary healthcare institutions in both urban and rural areas, enabling residents to undergo necessary medical tests while reducing investment costs.
In recent years, point-of-care testing (POCT) has been progressively implemented in community health institutions, playing a significant role in public health services such as disease prevention and control and health screening, as well as in primary diagnosis and treatment of common and frequently occurring diseases, and in the management and tiered assessment follow-up of chronic diseases. The decentralization of testing services to primary care settings under the tiered diagnosis and treatment model will drive the development of various POCT sub-sectors and substantially expand the demand for POCT products. Meanwhile, some routine tests that are cumbersome and time-consuming in large hospitals will also be replaced by POCT.
Portable Medical Devices
Family doctor teams can provide home visits; therefore, following the expansion of team sizes, portable medical devices will experience explosive growth. Portable medical devices such as blood pressure monitors, blood glucose meters, portable automated external defibrillators (AEDs), portable ECG monitors, and simple respirators will see significant opportunities, facilitating their transport by family doctors to patients’ homes.
In the "Administrative Measures for the Construction of National Demonstration Zones for Comprehensive Prevention and Control of Chronic Diseases," community health service centers and township health centers are required to provide services such as blood glucose testing, blood lipid testing, simple pulmonary function testing, and fecal occult blood testing, and to carry out screening and early diagnosis of major chronic diseases including cardiovascular and cerebrovascular diseases, key cancers, diabetes, and chronic obstructive pulmonary disease. To deliver these services at the primary care level without the widespread procurement of large-scale diagnostic equipment, portable medical devices play a significant role in enabling early screening and follow-up evaluation.
As patients with chronic conditions such as hypertension and diabetes will be key focus areas in the “roadmap” for tiered diagnosis and treatment, primary healthcare institutions will be responsible for the initial clinical diagnosis and long-term management of these two diseases, making blood pressure monitors and glucose meters essential medical devices. Wearable devices capable of measuring vital signs such as heart rate and blood pressure, as well as monitoring nighttime sleep patterns, will also gain favor among primary healthcare institutions.
With the preliminary establishment of the primary healthcare system and the tiered diagnosis and treatment system, third-party service providers such as independent clinical laboratories and independent medical imaging centers will benefit significantly, as collaborations with them by primary healthcare institutions are increasingly growing.
Third-party medical testing laboratories refer to healthcare institutions that, under the license of health administrative departments, possess independent legal entity status, operate independently from hospitals, engage in clinical laboratory testing or pathological diagnosis and services, and can independently assume liability. The services they provide differ from those of ordinary healthcare institutions; they do not treat patients. Their clients are hospitals, clinics, and community health service centers, and they primarily provide medical laboratory testing and pathological examination.
As the demand for clinical laboratory services continues to expand across healthcare institutions at all levels, and as medical resources become more decentralized, the third-party medical testing industry and third-party imaging centers are poised for substantial market growth. However, the third-party testing market driven by family physicians has a distinct characteristic: the tests offered tend to be less complex, focusing primarily on routine monitoring for patients with stable chronic conditions. Compared with the long queues at tertiary hospitals, rapid and convenient third-party testing remains an attractive option.
Currently, third-party medical testing institutions in China face challenges such as limited service offerings, small enterprise scale, and an insufficient range of test items. For county-level and lower-tier hospitals, establishing a medical testing center of considerable scale is impractical, as it would entail not only the procurement of expensive testing equipment and reagents but also the training of specialized personnel and recruitment of talent.
Third-party remote medical imaging diagnostic centers are also an important pathway to achieving tiered diagnosis and treatment, and they will find their own room for development in the promotion of primary healthcare. There are many similar third-party services. By the end of 2016, the National Health and Family Planning Commission successively issued basic standards and management regulations for four categories of independently established medical institutions: medical imaging diagnostic centers, medical laboratories, blood purification institutions, and pathology diagnostic centers. Such third-party medical service institutions can, to a certain extent, alleviate the problem of uneven resource allocation. The National Health and Family Planning Commission encourages social forces to actively participate in establishing independently set-up medical institutions and to develop towards group-based and chain-operated models.
The grassroots market will be the primary driver of pharmaceutical consumption in the coming years and a true test of corporate competitiveness. However, the supporting mechanisms and related systems for the current grassroots pharmaceutical market remain highly underdeveloped. Drug procurement has not yet met the standards for standardized procurement and usage stipulated in national policy documents, nor have relevant policies and regulations been fully and comprehensively implemented. The grassroots market is characterized by dispersed terminal outlets, low purchasing power per site, small order values, diverse procurement channels, high distribution costs, limited medical infrastructure and treatment capabilities at the primary care level, a narrow range of available drug varieties, lower drug prices compared to urban hospitals, and a predominance of lower-tier medications.
To establish a firm foothold in the grassroots pharmaceutical market, it is essential to integrate the two critical links of distribution and terminal sales, build a sales network, and extend sales channels down to the county, township, and village levels. At the same time, companies must deploy sufficient personnel to cover terminal outlets and effectively manage key elements such as product portfolio, market access, sales force, sales expenses, policy adaptation, and management mechanisms, thereby increasing the likelihood of capturing the grassroots market. For large pharmaceutical distribution enterprises, the “reshuffling” of the grassroots pharmaceutical distribution market has also accelerated distribution reforms.
Strengthening primary care as the first point of contact and implementing a tiered diagnosis and treatment system will channel more patients to primary care facilities, leading to an increase in patient visits and a growing number of chronic disease patients. Moreover, national policies will liberalize the baselineLong-term prescriptions for chronic diseases at primary care institutions will significantly increase the volume of chronic disease medications at the grassroots level. Emphasis on the primary care market, with strong sales channel management and extensive terminal coverage.enterprises will gain greater room for development.
“Minor illnesses treated in the community, major illnesses referred to hospitals”—this is the tiered diagnosis and treatment model advocated by the new healthcare reform. However, patients face difficulties accessing care at large hospitals, while small clinics struggle to earn trust. The future trend will see tertiary hospitals focusing on critical cases, with outpatient services shifting toward primary care providers. In addition to community health service centers, primary healthcare also includes privately funded individual clinics and chain medical institutions. Individual clinics, which belong to the primary care market, have previously experienced unregulated growth; many remain stuck at 1990s standards, suffer from poor operational performance, and lack support for physician development. Standalone independent clinics will find survival increasingly difficult, making branding, scaling, standardization, and chain operations an inevitable trend. Consequently, some private enterprises have begun to establish chain clinics, entering the blue ocean of primary healthcare.
Chain clinics can provide unified management standards, software systems, and management of physicians practicing at multiple locations. They can also offer family doctor contract services, chronic disease management, and invite specialists for consultations, thereby delivering better services to residents. This type of branded, scaled, and standardized chain clinic represents the future development trend of primary healthcare and is attempting to tap into the vast primary care market. Currently, there are few primary healthcare institutions capable of meeting the demand for high-quality medical services, which has led to a significant migration of patient visits to tertiary hospitals. If private chain clinics can address these issues, they will be able to accommodate a substantial portion of this patient demand.
For primary healthcare, building a "Healthy China" requires a shift from being "disease-centered" to "people's health-centered," with the core of this transformation lying in enhancing the service capabilities of primary healthcare institutions. With the advent of population aging in China and rising household incomes, the primary healthcare market holds immense potential.
This article analyzes the benefits that the national promotion of tiered diagnosis and treatment will bring to niche sectors related to primary healthcare institutions. In the next article, VCBeat will compile a list of companies in its database that are already involved in primary healthcare, examining how these enterprises serve the sector.
Primary HealthcareUnderstanding Primary Healthcare Here
Focusing on Reporting the Industrial Transformation Brought by New Technologies Empowering Primary Healthcare
Welcome to follow the WeChat account of Primary Healthcare by scanning the QR code. For reprints on websites, official accounts, etc., please contact liu.zy@vcbeat.top for authorization.
