Dentist Nelson Wood Files IPO Prospectus: Pioneering Opioid-Free Pain Management in Dental Care

In the U.S. healthcare sector, the use of opioids has sparked considerable controversy and ongoing turmoil. Yet dentist Nelson Wood has adopted a unique approach, eschewing opioids for pain management in favor of alternative medications grounded in new pharmacological and clinical knowledge. How have patients and the dental community responded to this outcome, and what insights does it offer us?
Nelson Wood once operated a dental clinic in Hyannis. But the dentist was involved in a disgraceful deal: he prescribed opioids to some patients and then had them share some of the pills with him to satisfy his addiction.
Wood’s illicit dealings came to an abrupt halt when he was arrested in a gym parking lot while engaging in drug transactions with a patient with whom he had reached an agreement. This scandal occurred nearly a decade ago in Western Massachusetts. Since then, Wood has undergone addiction treatment, regained his dental license, and diligently resisted any temptations that could lead to relapse; nevertheless, the scandal nearly destroyed his career. He later even petitioned the government to revoke his authority to prescribe potent opioid medications—such as Percocet, Vicodin, and OxyContin—which are classified as “drugs with a high potential for abuse.”
Wood believed that the beneficial efforts he was attempting were not just for himself, but also for his patients. However, this conflicted with the current state of the industry,Because the dental industry has a deeply entrenched culture of opioid use, and his attempts were also detrimental to the industry’s commercial interests.。
It is difficult for many dentists to change their entrenched traditional mindset and adopt alternative medications that incorporate new pharmacological and clinical knowledge. As healthcare providers, they are always cautious, striving to use only those drugs with which they are familiar and confident. While this attitude is understandable, it may not fully benefit patients.
Wood’s story serves as an excellent case study for examining the pressures dentists face when prescribing analgesics.Although studies have shown that most dental patients only take over-the-counter pain relievers such as ibuprofen, many patients undergoing tooth extraction or root canal therapy still expect their dentists to prescribe stronger analgesics.。
The pressures facing Wood extended far beyond anxious patients; a major insurance company had hesitated to include him in its provider network due to his restricted prescriptive authority.
“It’s as if they insist that I prescribe opioids,” Wood said in an interview with STAT. “Drug addiction is tearing this country apart, yet people want me to fuel that trend. I say clearly, ‘No, I won’t do it—absolutely not.’”
Although opioid analgesics play a crucial role in pain management, they are also highly susceptible to abuse by individuals with substance use disorders. Most individuals who misuse opioids have previously been prescribed these medications themselves, or their friends or family members have received such prescriptions.Dentists have now become a major source of opioid prescriptions, particularly for young patients undergoing wisdom tooth extraction.
According to statistics from government researchers, dentists prescribe approximately 8% of all opioid prescriptions in the United States, yet they rank highest in prescribing opioids to adolescents, accounting for 30.8% of all opioid prescriptions for patients aged 10–19, which involves approximately 700,000 individuals. From 1994 to 2007, the number of controlled substance prescriptions, including opioids, issued to adolescents nearly doubled. Of particular concern is that this age group is most susceptible to drug abuse and addiction.
Dr. Paul Moore, Professor of Dentistry and Pharmacology at the University of Pittsburgh, stated, “In fact, most patients can tolerate pain even without the use of opioid analgesics,”For instance, we found that the combination of Advil and Tylenol can significantly alleviate pain with fewer adverse reactions. 。”
He also stated that prescription painkillers such as Percocet and Vicodin are not very effective in treating acute dental pain and are often accompanied by side effects, such as nausea, not to mention the risk of addiction.
In a study, 350 cases among 35,000 participants were examined to analyze the adverse reactions of analgesics, with a placebo group serving as the control. The results showed that for most drug combinations, such as most nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, and analgesic combinations excluding opioid components (e.g., codeine), the incidence of adverse reactions was similar to that in the placebo group.
However, opioid analgesics or combination medications containing opioids result in more adverse reactions than the placebo group. The combination of ibuprofen and acetaminophen produces fewer adverse reactions than the placebo group.Since the participants in this study were predominantly healthy young adults who rarely used analgesics, the results may differ among older, less healthy individuals or those who take painkillers long-term.
Dr. Moore also noted that there is a growing call to reduce opioid prescriptions in dentistry. He acknowledged that two dentists have already chosen to operate their practices without any license from the Substance Abuse and Mental Health Services Administration, which means they are running their clinics without prescribing pain medication to patients.
From 2007 to 2012, the proportion of opioid prescriptions issued by U.S. dentists decreased by 6%.In October 2016, the American Dental Association issued a statement on opioid use, recommending that dentists consider using over-the-counter analgesics, such as Motrin and Advil, as “first-line treatment options for acute pain.”。
However, as Wood has indicated, pain management practices in the dental industry are unlikely to change anytime soon.
Is it necessary to take 30 painkillers after tooth extraction?
In 2014, the U.S. Drug Enforcement Administration (DEA) began to strengthen regulation of opioid prescriptions; however, many leading dental associations united to challenge this proposal, although their efforts were ultimately unsuccessful.Six groups representing dentists and oral surgeons, including the American Dental Association, agree that restrictions on opioids will exacerbate patients’ pain.Dr. David Keith, an oral and maxillofacial surgeon at Massachusetts General Hospital, stated that this reflects physicians’ professional inertia. He co-chaired a panel that recommended providing additional training on preventing opioid misuse to dental students in Massachusetts. “We should try to shift the focus of the proposal,” said Dr. Keith.
Dr. Brian Bateman, an Associate Professor of Anesthesiology at Harvard Medical School, who is dedicated to studying opioid use following tooth extraction, stated that many dentists prescribe “massive” amounts of opioids for patients after tooth extraction, which often far exceeds patients’ own expectations. In many cases, dentists prescribe 20 to 30 opioid analgesic tablets; however, in reality, many patients require only a small quantity of pain medication before their pain completely subsides.
Dr. Bateman is deeply concerned, as the unused pain medications left over by patients are highly susceptible to misuse. Dr. David Keith represents a category of physicians who estimate that they can prescribe up to 30 million painkiller pills to patients annually.
Keith noted that opioid prescriptions are so commonplace in the dental industry that dental journals feature numerous advertisements for medications used to manage opioid-related side effects, such as nausea and vomiting.
The dental community firmly believes that opioid medications such as Vicodin are far more effective than over-the-counter drugs; however, mounting evidence to the contrary indicates otherwise, and external pressure on this issue is increasingly intensifying.Some insurance companies and hospital systems take into account complaints from patients who were not prescribed opioids when reviewing dentists’ performance. Some patients, if not given an opioid prescription, may angrily denounce dentists on social media for disregarding their pain, which could significantly damage the reputation of clinics that have attempted to reduce opioid prescribing.
Dr. Moore said that after a lecture in Montana, a dentist told him that while he was well aware that many patients did not actually need opioids, he would still prescribe them. “He told me he had reviewed my data and acknowledged that I was absolutely right,” Dr. Moore added. “But he also said that there were only three dental clinics in his area, and if he gained a reputation for not prescribing opioids to patients, he would not be able to survive in the industry.”
Wood, now 62, practices in a converted house near Hyannis Port, where he paces slowly each day. He single-handedly runs his clinic, working diligently six days a week. Years of alcohol and drug abuse have taken a severe toll on his health, and he also suffers from arthritis, with daily pain in his back and knees. He frequently takes smoke breaks during work hours, then sprays on cologne to mask the odor so that his patients do not notice. When asked whether he would consider using opioids to alleviate his pain, he honestly admitted that the temptation was strong. Although he could easily obtain opioid prescriptions from other physicians for pain relief, he would never do so.
Wood’s situation is precarious; his struggle with substance abuse has drained him of significant financial resources and energy. His dental license was once suspended, he lost his home, and he has been arrested on multiple occasions.
Wood grew up in Brookline, a suburb of Boston. He first misused drugs at the age of 13 and later developed alcoholism. His parents were survivors of the Auschwitz concentration camp. His father, who ran a construction company, was an emotionally distant and chronic alcoholic. Other members of his family also struggled with addiction.
When Wood was 20 years old, he was arrested in a DEA cocaine investigation, but he avoided imprisonment by participating in drug rehabilitation treatment. Since then, he has been trapped in a vicious cycle of struggling with substance abuse and alcoholism, repeatedly achieving sobriety only to relapse.
After obtaining his dental degree from the University of Pennsylvania, he joined a renowned dental clinic in Boston. However, in 1992, based on an investigative report, police investigated him for inappropriate prescribing of Percocet, Valium, and Xanax, leading the American Dental Association to place him on a five-year probationary period.
By 1999, after another episode of drug abuse, Wood left the dental profession and took a position at a medical institution in Mississippi. The best job he could find at the time was working as a cashier at a supermarket, earning $7.20 per hour. A few months later, he participated in a research project at the University of Mississippi, where his role involved cleaning dogs’ teeth, for which he was paid $50 per dog.
In 2006, Wood returned to Massachusetts and opened a denture laboratory there. However, he admitted that his addiction quickly relapsed after he was prescribed painkillers following a surgical procedure. In 2007, as mentioned at the beginning of the article, he was arrested in a gym parking lot while engaging in drug transactions with a patient. Rumor has it that Wood reached an agreement with a couple who were his patients: he would write prescriptions for Vicodin and Percocet for them in exchange for some of their pills for his own use.
He subsequently entered the Massachusetts Physician Health Program, a medical initiative specifically designed for healthcare professionals struggling with substance use disorders. He praised the program, stating that it had essentially saved his life. Under the close supervision of the Drug Enforcement Administration (DEA), the American Dental Association, and the program itself, Wood reported that he was able to effectively manage his addiction and has remained in remission since 2008.
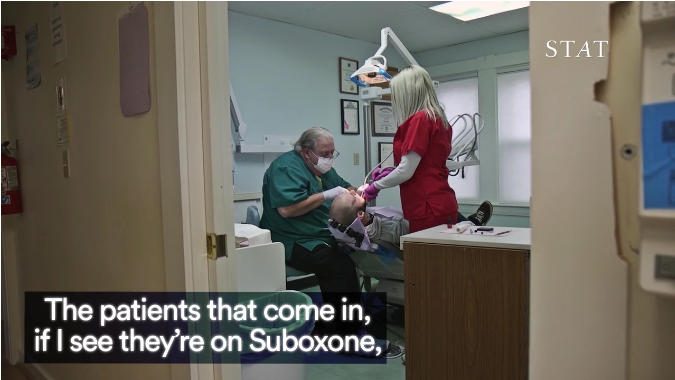
Wood is communicating with and treating a patient with drug addiction.
In 2011, Wood stumbled upon a notice that a dental practice in Cape Cod was for sale. He seized the opportunity, borrowing money from his brother to pay the down payment and purchase the clinic. Later, two DEA agents visited his practice and informed him that he was now eligible to have his full prescribing privileges reinstated. However, Wood told them that he only wanted a license with limited prescribing authority, as having the power to prescribe medications such as Vicodin or Percocet would pose a significant temptation that needed to be guarded against. Despite the restrictions on his prescribing privileges, he could still provide patients with milder analgesics, thereby reducing the likelihood of drug abuse.
Wood resignedly stated that his past history of drug addiction, coupled with his current refusal to prescribe highly addictive opioid medications to patients, has led insurance companies to view him with caution.Blue Cross Blue Shield of Massachusetts approved Wood’s inclusion in its insurance network only after conducting a prolonged review of his credentials. Wood stated that the physician responsible for reviewing his case informed him that, generally speaking, insurers do not trust dentists who lack a full DEA registration. To address the insurer’s concerns, Wood explained that he had arranged for physicians in the local hospital’s emergency department to prescribe opioid medications to patients in need.
Blue Cross has refused to discuss the specific case of Dr. Wood with us. The company stated that, generally speaking, they evaluate each dentist’s situation on a case-by-case basis, but the type of license held by the dentist, as issued by the DEA, is an important consideration.
Last month, Guardian Life Insurance Company notified Wood that he would not be included in their insurance network due to his past record of having his dental license revoked.
Wood stated that the majority of his patients are covered by Medicaid, a public insurance program primarily serving low-income individuals, while some patients opt to pay out-of-pocket. The remaining quarter of his patients are covered by several private insurance companies that include Wood in their provider networks.
Another reason Wood deliberately restricted his prescribing authority was that he did not want to become a target for drug addicts.
Cape Cod, where he is based, is renowned for its beautiful beaches and as the site of the Kennedy family’s summer homes, yet it is simultaneously grappling with a rampant opioid crisis.Massachusetts is the seventh-highest state in the U.S. for mortality rates due to the drug epidemic; in 2015, 1,724 people in the state died from drug abuse, with the death toll continuing to rise in recent years, representing a 35.3% increase from 2014.In particular, the rate of substance abuse in the Cape Cod region is higher than that in urban areas of the state, such as Boston.
Just last month, police dismantled a fentanyl (a narcotic drug) trafficking ring here, which was rumored to be controlled by the prominent Shriver family, with transaction volumes exceeding millions of dollars.
Opioid addicts easily found their way to Wood’s door. A young patient who visited shortly after Wood reopened his clinic complained of a toothache. After examining him, Wood advised that the tooth needed extraction, but the patient was unwilling. He told Wood that he simply wanted some oxycodone to alleviate the pain. However, as oxycodone is an opioid prescription medication for which Wood did not have prescribing authority, Wood informed the young man that he did not need such medication. Wood later noticed that the patient appeared to be signaling someone outside. He then discovered the man’s girlfriend attempting to enter through the clinic’s back door, likely in search of opioids. Wood circled around to the back entrance and apprehended her.
Following that incident, Wood posted a sign in the clinic’s reception area that read: “Our clinic does not prescribe or dispense opioid medications.”
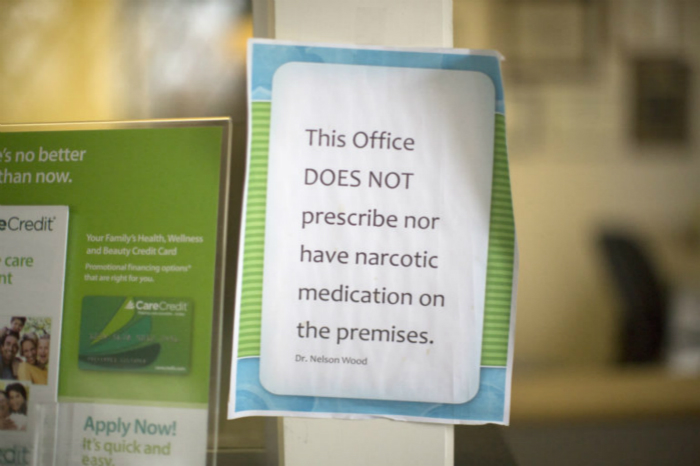
No prescriptions issued, and no opioid medication display signs provided.
On another occasion, a mother brought her daughter to seek medical attention, and Wood prescribed a milder painkiller for the daughter. After the daughter left, however, the mother rushed into Wood’s office demanding a stronger prescription. “Clearly,” Wood remarked, “the mother was simply trying to obtain opioids for herself.” Wood also mentioned that some patients had offered sexual favors in exchange for opioid prescriptions, but he refused. In even more extreme cases, individuals altered the Valium dosage on prescriptions from 4 to 24.
Over the past year, three dental clinics located within two miles of Wood’s clinic have had their licenses revoked or faced arrest due to improper opioid prescribing.These developments also directly prove that Wood is doing the right thing.
“I don’t want my mind to feel like a hamster running on a wheel every time I’m in excruciating pain, constantly plotting to use my medical license as an escape,” Wood said.
In contrast to the clinic’s initial days, when it saw barely any patients, Wood now sees hundreds of regular patients each day. He notes that many of his patients are fully aware of his past. Some share with him their own or their family members’ struggles with substance addiction, and a few have even died from drug misuse. These experiences serve as a stark reminder to Wood: if he were to use these highly addictive substances again, his medical license, his clinic, and the redemption he is striving for would all vanish into thin air.
“If I don’t stay sober, I will lose everything,” Wood admitted. “But I am determined to remain sober, as I have relapsed before and twice lost everything.”
Source: STAT
Author: DAVID ARMSTRONG