Comprehensive Report on Telemedicine Policies Across All 50 U.S. States
The Chinese version of this report was jointly produced and released by VCBeat and the Global Doctors Organization.
Telemedicine refers to a novel healthcare service that leverages computer, remote sensing, telemetry, and remote control technologies to fully utilize the medical expertise and equipment advantages of large hospitals or specialized medical centers. It provides remote diagnosis, treatment, and consultation for patients in remote areas with limited medical resources, aiming to improve diagnostic and medical standards, reduce healthcare costs, and meet the health needs of the general population. Telemedicine was first applied by American scholars in the late 1950s and has undergone 60 years of development, making the United States one of the most advanced countries in telemedicine globally. In China, the maturation of telemedicine is a prerequisite for implementing the national strategy of tiered diagnosis and treatment.
In February 2017, the American Telemedicine Association (ATA) released the report “Gap Analysis of Telehealth Across All 50 States,” presenting detailed data on telehealth coverage and reimbursement policies in each U.S. state. Although progress has been slow in some states, the overall implementation of telehealth across the country is improving. VCBeat (WeChat ID: vcbeat) has provided a full translation and compilation of the report’s content to offer readers an in-depth understanding of the current state of telehealth in the United States.
The American Telemedicine Association (ATA), established in 1993, is a non-profit, membership-based association headquartered in Washington, D.C. As a leader in telemedicine, the ATA aims to improve healthcare by enhancing the quality, equity, and affordability of medical services worldwide. It boasts a network of more than 10,000 industry leaders and healthcare experts. The ATA hosts premier telemedicine conferences, as well as trade exhibitions focused on technological innovation and networking.
The report released by the ATA revised two policies of the state government, identifying gaps in telehealth coverage, reimbursement, physician practice standards, and licensure.
The report employed 13 metrics related to coverage and reimbursement, noting that “despite decades of positive and significant findings from clinical empirical research and increased utilization of telemedicine, national healthcare policies remain unstable.”
Latoya Thomas, Director of the ATA National Policy Resource Center, stated in a press release, “This is encouraging news for patients, providers, and businesses leveraging telehealth and other digital health platforms. These reports indicate that insurers, state legislators, and Medicaid agencies view telehealth and other digital health platforms as affordable and convenient solutions to address provider shortages and improve patient access to high-quality healthcare.”
Reimbursement and coverage for telemedicine services represent one of the greatest challenges in the application of telemedicine.. Complex insurance clauses and varied payment processes often become the main obstacles for patients and healthcare providers in utilizing telemedicine.
The American Telemedicine Association (ATA) has compiled 50 distinct and complex telehealth policies from all 50 U.S. states and converted them into a simple, user-friendly format. VCBeat has learned that this report also analyzes disparities in telehealth across states, including state-specific standards of medical practice and licensure, as well as telehealth coverage and reimbursement criteria. The core issues the report aims to address include:
• “How do this state’s policies promoting the adoption of telemedicine compare with those of other states?”
• “How should this state improve policies to promote the adoption of telemedicine?”
This report categorizes coverage and reimbursement-related data into 13 metrics, revealing the development and stagnation of telemedicine across different states under varying policies through analysis.
Since the American Telemedicine Association (ATA) released its inaugural report in September 2014, all Medicaid programs across the United States have adopted some form of telehealth coverage. Furthermore, since the 2016 report, seven states have implemented policies to improve telehealth coverage and reimbursement; meanwhile, two other states and the District of Columbia have chosen to reduce telehealth coverage or impose further restrictions on it (Figure 1).

As shown in Figure 2, states have made relentless efforts in recent years to ensure equitable coverage under private insurance, state employee health plans, and/or Medicaid programs by eliminating restrictive clauses and enacting relevant legislation. Overall, no state received a failing composite score; an increasing number of states now achieve “A” or “B” ratings, which are above the national average. Notably, compared with the analysis conducted in December 2015, Connecticut and Rhode Island have improved their ratings from “F” to “B.”
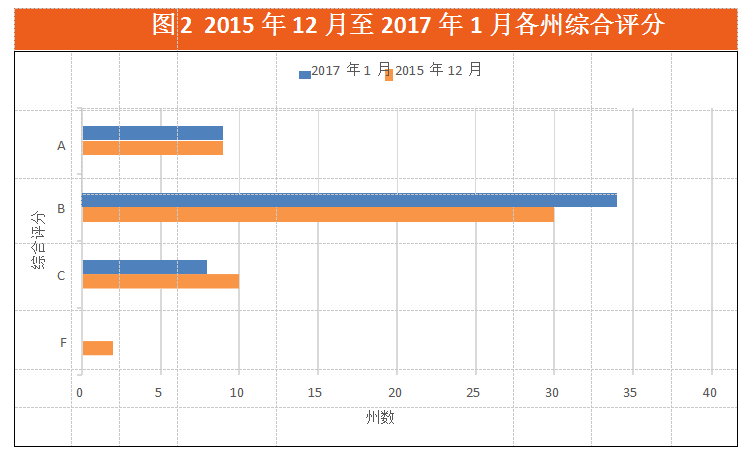
This year, Connecticut, Florida, Hawaii, Idaho, Rhode Island, Utah, and West Virginia achieved higher scores, indicating that these states have policy environments supportive of telehealth applications. In contrast, the overall scores for Texas, Delaware, and South Carolina declined. South Carolina’s rating dropped from a “B” to a “C,” primarily because the state’s “Home and Community-Based Services” waiver, which allowed remote patient monitoring via telehealth, has expired (Table 1).

When we categorize the data into 13 indicators,VCBeat has found that,Data across states show greater variation.
• Since the first report in 2014, 10 states have enacted telehealth parity laws. Among the 31 states that have passed private insurance parity provisions for telehealth, 24 states and the District of Columbia received the highest scores, indicating that their parity policies cover the entire state without any restrictions on providers or technologies (Figure 3). Fewer than half of the states nationwide (20 states) ranked lower and received failing grades.The reason can be attributed to the absence of equality laws or the establishment of numerous artificial barriers.. The adoption of parity laws represents a significant step forward. Arkansas’s grade remains failing, as it is the only state with a parity law that mandates in-person patient consultations.
• Telemedicine is already operational within Medicaid programs.All 50 U.S. states’ Medicaid programs cover certain types of telehealth services.. Eleven states have adopted more comprehensive telehealth coverage, providing patients with virtually barrier-free access to telemedicine services and achieving high scores in the overall assessment (Figure 4).Connecticut, Florida, Hawaii, and Iowa have ensured equitable coverage for telemedicine through reforms, leaving little to no restrictions on its use, while Rhode Island has also covered certain telemedicine services under its Medicaid program.VCBeat has learned that New Hampshire is the only state in the New England region to receive a failing grade and rank low, due to its Medicaid telehealth regulations adopting language similar to the restrictive provisions found in Medicare.
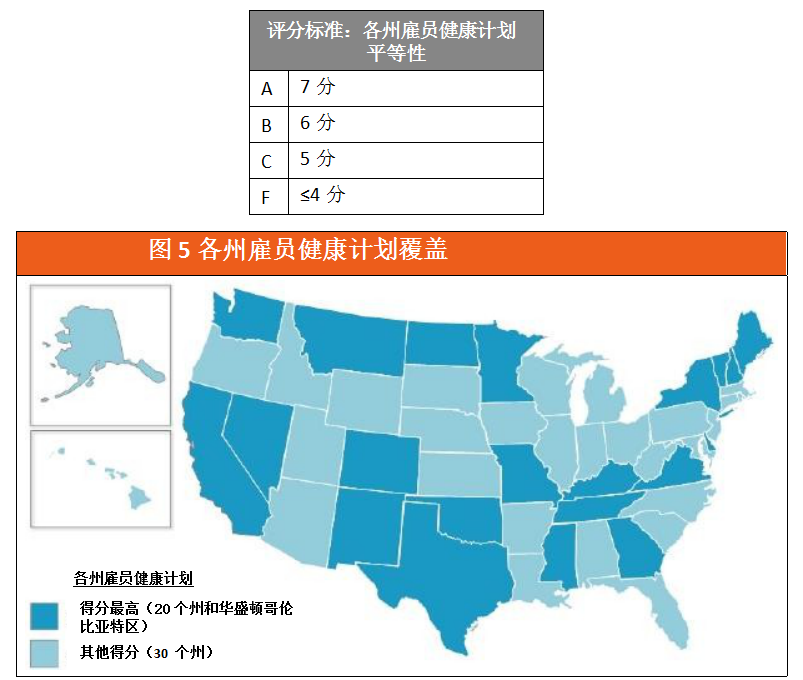
• Another area for improvement is telehealth coverage and reimbursement under state employee health plans. Twenty-six states have implemented one or more state employee health plans that cover some type of telehealth services. Most states self-insure their state employee health plans; therefore, the parity provisions applicable to traditional private insurers do not automatically apply to them. Due to partial or no coverage of telehealth, approximately 50% of states nationwide rank low and receive failing scores (Figure 5).
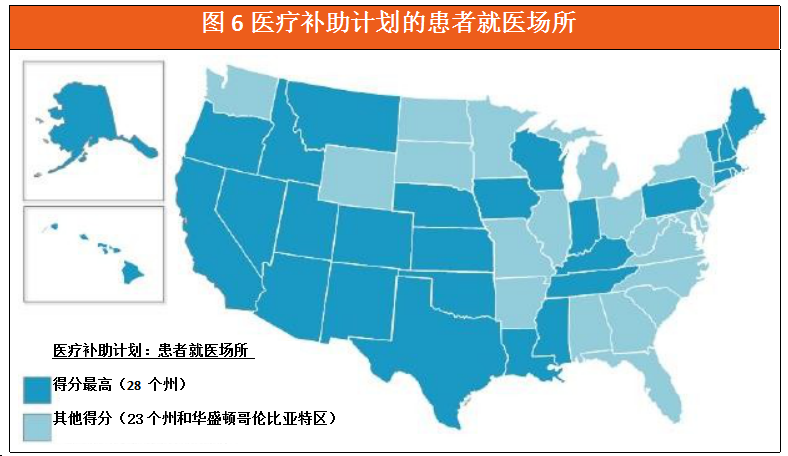
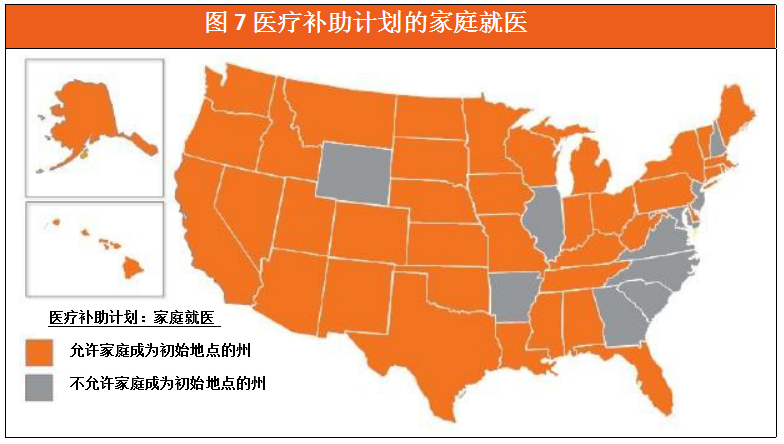
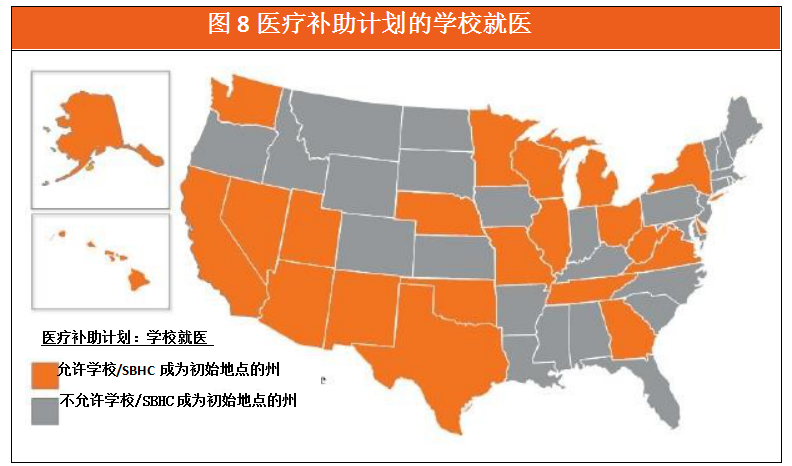
Regarding Medicaid programs, states continue to move away from the traditional “hub-and-spoke” model and allow the application of various new medical technologies. Twenty-eight states do not condition telemedicine reimbursement on the patient’s site of care (Figure 6). In addition,40 states recognize the family as the initial point of care, while 23 states and the District of Columbia recognize schools and/or school-based health centers as the initial point of care.(Figures 7-8).
More states, including Hawaii, Louisiana, and Nebraska, areEnable Medicare coverage for remote monitoring in chronic disease management through legislation or by seeking federal waivers.Currently, 21 states have achieved coverage for remote patient monitoring, and 15 states have covered store-and-forward technologies. Approximately half of the states nationwide rank low and receive failing scores because they only cover and reimburse telemedicine services delivered via synchronous platforms. Furthermore, despite the widespread adoption of smartphones across the United States, Idaho, Missouri, New York, North Carolina, and South Carolina still prohibit the use of “smartphone video” to facilitate telemedicine applications (Figure 9).
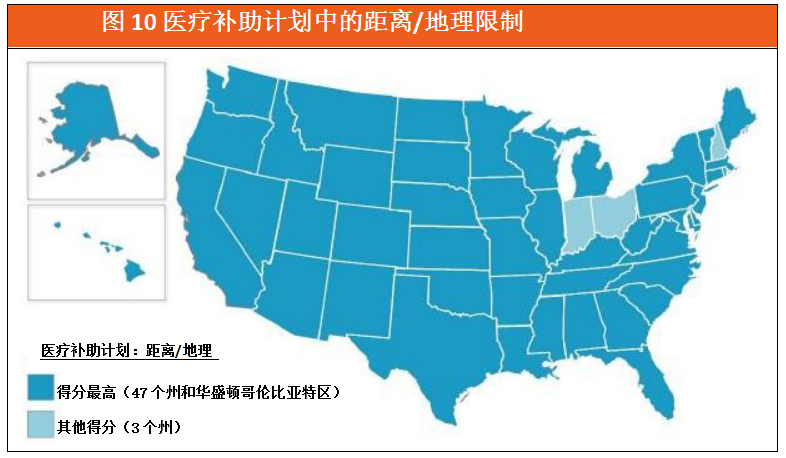
There is also a nationwide trend,That is, rather than focusing solely on rural areas or specified mileage requirements, it allows telemedicine to be covered under state Medicaid programs.(Figure 10). This is consistent with VCBeat’s previous expectations.
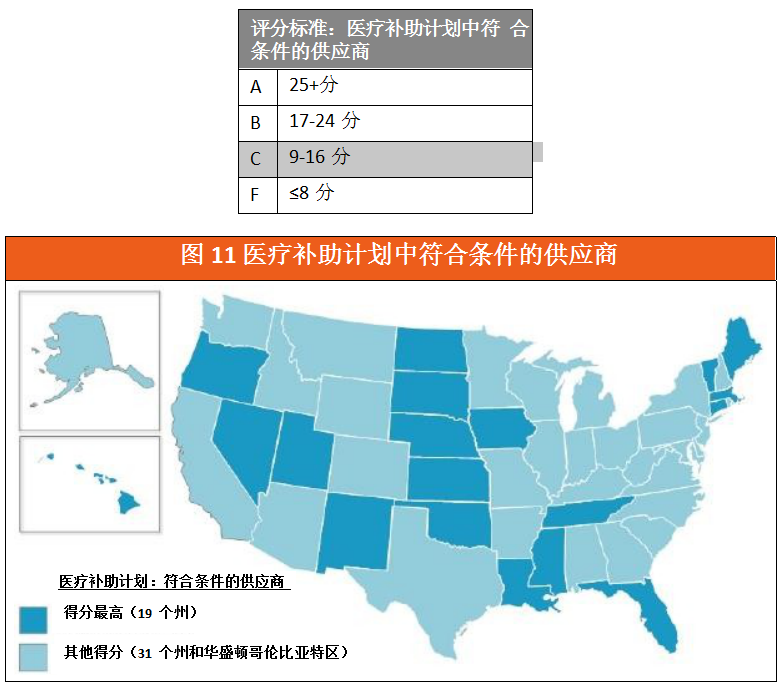
States are also increasingly leveraging telehealth to bridge provider shortages, ensuring patients have access to specialized medical services, including dental care and treatment or counseling for substance use disorders.Regarding reimbursement for telehealth services, 19 states do not specify particular types of telehealth providers (Figure 11); meanwhile, 16 states and the District of Columbia rank lower with failing scores, as they authorize fewer than nine types of telehealth providers. Montana is the only state that authorizes physicians exclusively as qualified telehealth service providers.
Overall, the scope of telemedicine professional services covered under Medicaid varies by state, with no two states having identical provisions.
• 13 states scored high in the coverage of physicians available to provide telemedicine services,However, most states only cover outpatient visits or consultations, and telemedicine services such as ultrasound and echocardiography have low coverage rates in these states.(Figure 12).
• For mental and behavioral health services,Generally, mental health assessments, individual therapy, psychiatric diagnostic consultations, and medication management are the most widely covered telehealth services.Fifteen states have high coverage of telemedicine services for mental and behavioral health (Figure 13). States with higher scores, such as West Virginia, encourage relevant institutions to use telemedicine to provide mental health services. In terms of mental health services, New York State ranks last due to regulations that impose restrictions on the provision of telemedicine services.
• Although the scope and applicability of policies vary by state,However, three states have expanded telehealth coverage to include remote rehabilitation services.. It is known that 25 states provide reimbursement for telerehabilitation services, among which 14 states rank high in coverage of telemedicine therapeutic services (Figure 14).
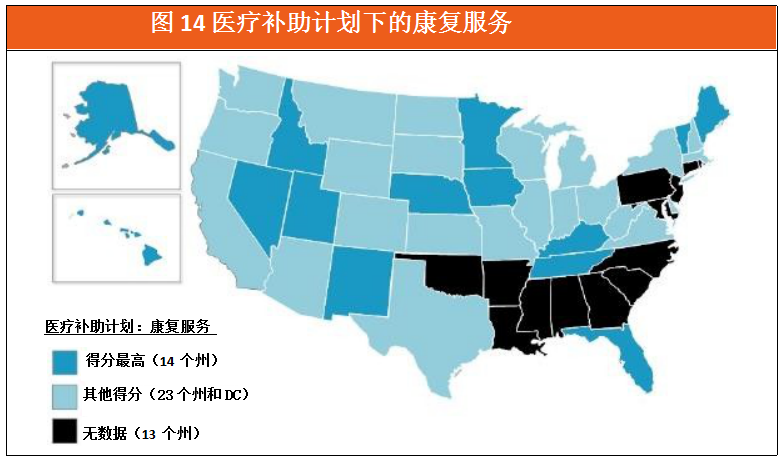
• Alaska and Hawaii are the highest-scoring states in the ranking of telehealth offerings under home health benefits (Figure 15). In this category, 70% of states nationwide received failing grades due to the lack of telehealth coverage under home health benefits.
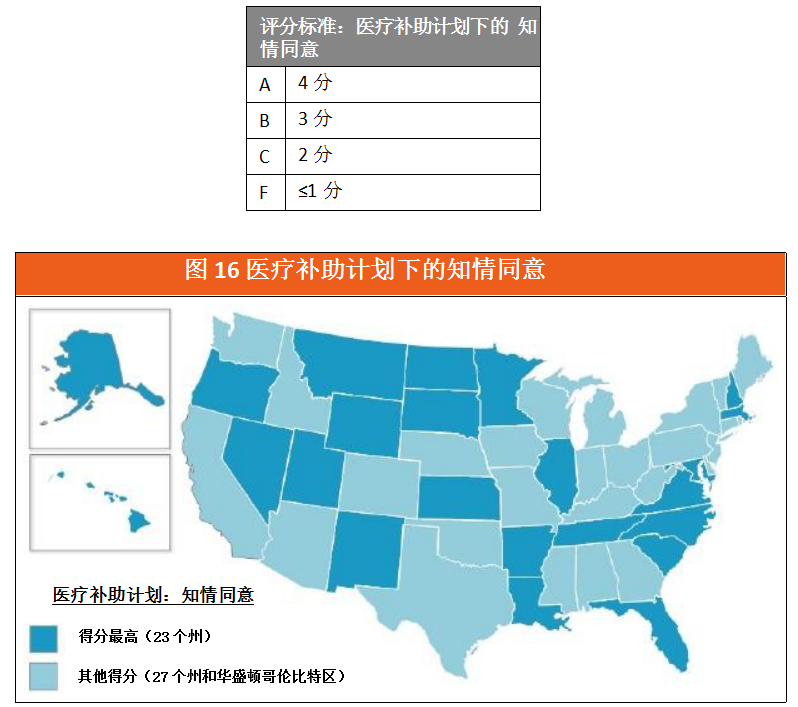
Finally, VCBeat found that 27 states and the District of Columbia have enacted specific patient informed consent requirements for the use of telemedicine (Figure 16). More states are planning to revise requirements regarding “telepresenters.” Thirty-four states do not require the presence of a “telepresenter” device during telemedicine services or at the service location (Figure 17).
Patients and healthcare providers across the United States are eager to understand how their state’s telehealth landscape compares with those of other states. Although numerous resources have elaborated in detail on each state’s telehealth policies, there is currently no literature offering a systematic, state-by-state comparison. To address this gap, the American Telemedicine Association (ATA) has developed a tool to clarify policy disparities among states, aiming to encourage states to streamline their regulations, accelerate the development of telehealth, and ultimately improve healthcare quality while reducing costs.
This report fills this research gap by answering the following questions:
• “How does our state’s telehealth policy compare to those of other states?”
• “Which states have the best telemedicine coverage?”
• “Which states impose the most barriers to telehealth access for patients and providers?”
It is worth noting that,This report is not a “guide” on how telemedicine should be reimbursed, but rather a tool that can serve as a reference for all relevant parties and inform future policy-making.. The results presented in this report are based on information collected from state statutes, regulations, Medicaid program manuals/announcements/fee schedules, state employee handbooks, and other federal and state policies, representing ATA’s understanding and interpretation of each state’s policies.
Legislatures across all U.S. states are increasingly focusing on how telemedicine can serve their populations. Policymakers are consistently committed to addressing challenges such as healthcare delivery, cost containment, care coordination, and provider shortages, with many states leveraging telemedicine to achieve these objectives.
Over the past five years, the number of states that have enacted telehealth parity laws has also doubled; in these states, private insurers are required to provide coverage for telehealth services equivalent to that for in-person outpatient visits. Furthermore, Medicaid agencies are developing innovative payment and delivery models incorporating telehealth, enabling Medicaid programs across all U.S. states to cover certain types of telehealth services.
Legislation permitting access to healthcare services via telemedicine, along with revisions to the scope of existing policies, are key drivers in promoting the adoption of telemedicine.Both patients and healthcare providers have benefited from policy improvements, such as the enactment of the Telehealth Equity Act, the expansion of telehealth service coverage, and the removal of statutory and regulatory barriers to telehealth. Although some states have introduced model telehealth policies, they still lack adequate enforcement mechanisms and widespread awareness, resulting in relatively low provider participation and ultimately preventing these pioneering telehealth reforms from realizing their full potential.
This report also examines circumstances that fall outside the scope of current policies or hinder providers and patients from leveraging and benefiting from telemedicine, particularly phenomena such as geographic discrimination and restrictions imposed on care settings for both providers and patients, as well as on the types of technologies used in telemedicine.
Score
This report is divided into the following two major categories to comprehensively evaluate each state’s telehealth coverage and reimbursement policies:
• Equity in Health Plans
• Payment Conditions for the Medicaid Program
The above two major categories will be measured using 13 indicators. The selection of these indicators is based on the latest publicly available information compiled and published by state public sector agencies. On the basis of this information,We assign quantitative values based on qualitative characteristics such as the scope of telemedicine services, provider and patient eligibility, technology types, and payment conditions.; Furthermore, we scored each state based on the effectiveness of relevant indicators and used these scores to rank and compare the states for each indicator. Within the two major categories, there are 3 indicators for equity in health plans and 10 indicators for payment conditions in Medicaid programs.
Each indicator is scored on a scale of 1 to 35, with overall ratings categorized as A, B, C, and F. This report also includes a category,Namely, documenting the innovative telehealth payment and service delivery models implemented by each state.. In addition to the network-specialized nursing and correctional facilities supported by individual states, the report also documents federal subsidy programs and waiver policies that some states can leverage to enhance access to telehealth services.
(I) Equality
The Parity Law signifies that telehealth services are covered by insurance to the same extent as in-person services.Currently, VCBeat has learned that 31 states and the District of Columbia have enacted laws ensuring full parity for telemedicine. However, Alaska and Arizona have enacted only partial parity laws, which still impose specific regulations on insurance coverage for telemedicine by limiting reimbursable services to a pre-designated list. Since the inception of our report, some states’ parity laws have included restrictions on patient care settings. Therefore, this report adopts “parity” as one of its methodological frameworks and continues to assess other policy elements in each state that may either facilitate or hinder telemedicine parity within private insurance.
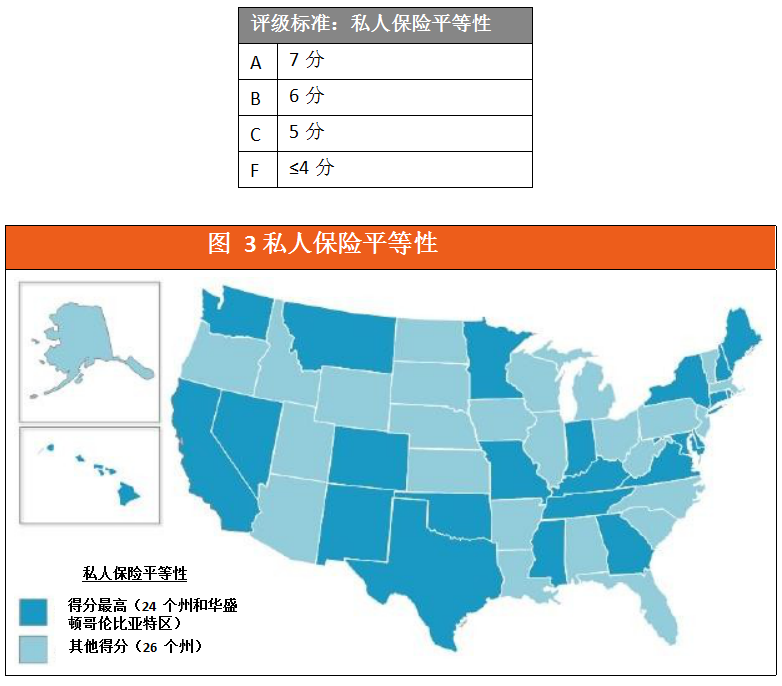
The states with the highest scores for parity in private insurance coverage for telemedicine are those that provide statewide coverage and impose no restrictions on providers, technology, or patient sites of care (Figure 3). This year, Rhode Island passed its 2016 parity law, propelling it into the ranks of states with high parity scores. Among other states that have enacted parity laws, Alaska and Vermont received mediocre scores (C); this is because Alaska’s parity law covers only mental health services, while Vermont’s legislators have imposed restrictions on patient sites of care.
Although Arizona has removed provisions that limited coverage to rural areas and began providing equitable telehealth services statewide, it continues to restrict the modalities of telehealth, covering only interactive audio and video delivery, and only under specific types of services and conditions. Despite enacting an parity law in March 2015, Arkansas still received a failing grade in this report’s scoring due to numerous restrictions on patient locations, provider types, and the requirement for an in-person visit to establish a provider-patient relationship. VCBeat found that 44% of states nationwide received a failing grade (F) in this report, a decrease compared to the initial report.
In the United States, each state’s Medicaid program is evaluated based on its restrictions regarding healthcare services and patient care settings.Furthermore, this report also examines state regulations on provider qualifications and technology types to determine whether each state has the capacity to fully leverage telehealth to overcome barriers to service delivery., and measured other content in the relevant policies of each state that could promote or hinder the equality of telemedicine services in the Medicaid program.
Medicaid programs in all states cover certain types of telehealth services.
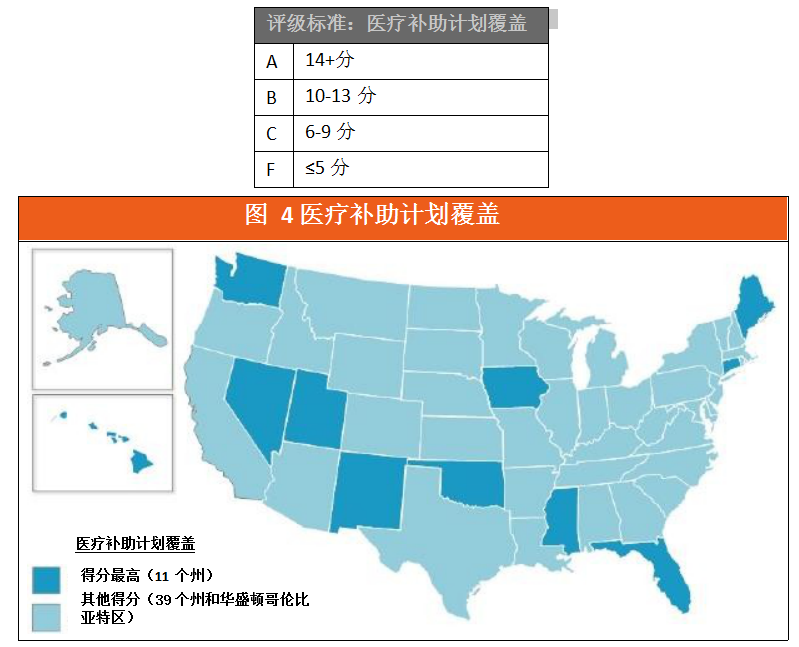
Telehealth services in 11 states received high scores under Medicaid programs (Figure 4). New Hampshire ranked last with a failing grade (F) because it still imposes restrictions on geographic location, scope of services, provider eligibility, and patient care settings. States such as Connecticut, Florida, Hawaii, Idaho, Utah, and West Virginia have improved and expanded telehealth coverage within their Medicaid programs. Rhode Island’s ranking surged after the state added telehealth to its Medicaid coverage, allowing reimbursement for certain initial and follow-up telehealth services.
C. State Employee Health Plans
We measured other provisions in state-level policies that could either advance or hinder equity in telehealth services within employee health plans across states.Most states have self-insured employee health plans, so the equal treatment clauses of traditional private insurance companies do not automatically affect them.However, Oregon is an exception, as the state amended its equal protection laws to include self-insured state employee health plans.
Twenty-six states, building on their passage of parity laws that expanded telehealth coverage, also provided partial coverage for telehealth under state employee health plans (Figure 5). North Dakota’s parity law covers only the state employee health plan. Approximately 50% of states ranked low and received failing scores due to partial or no coverage of telehealth.
(II) Medicaid Service Coverage & Payment Conditions
In telemedicine policies, the location where the patient is situated when receiving medical services is referred to as the originating site (correspondingly, the location of the provider is known as the distant site).Patient location remains a highly contentious issue in telehealth coverage. Traditionally, telehealth coverage has been defined by the requirement that patients receive medical services within specific types of healthcare facilities, such as hospitals or physician offices. With advances in remote computing capabilities (e.g., cloud processing) and mobile communication technologies (e.g., 5G wireless), current telehealth services can now cover patients regardless of their location, whether at home, in the workplace, at school, or elsewhere. In this report, we examine how each state’s Medicaid program has either relaxed or restricted coverage scope and reimbursement conditions for telehealth with respect to patient site of service. The following are the eligible patient locations identified in our analysis:
• Hospital
• Physician Outpatient Clinic
• Other Supplier Outpatient Clinics
• Dental Clinic
• Family
• Federally Qualified Health Center (FQHC)
• Critical Access Hospital (CAH)
• Rural Health Center (RHC)
• Community Mental Health Center (CMHC)
• The only community hospital
• School-Based Health Centers (SBHCs)
• Assisted Living Facilities (ALF)
• Skilled Nursing Facility (SNF)
• Stroke Center
• Rehabilitation/Dietary Therapy and Healthcare Institutions
• Outpatient Surgery Center
• Residential Treatment Center
• Health Department
• Dialysis Center
• Rehabilitation Center
• Pharmacy
One point is awarded if a state designates one of the aforementioned patient settings as an eligible originating site. If a state does not specify particular originating sites, it receives the maximum score of 21 points.
Among them, 28 states do not designate specific healthcare settings or locations for patients (Figure 6). In addition, 40 states allow homes to serve as the initial point of care for patients, while 23 states and the District of Columbia recognize schools and/or School-Based Health Centers (SBHCs) as initial points of care (Figures 7–8). Illinois, New Jersey, and North Dakota received the lowest rankings and failing grades (F) because they designated fewer than six initial points of care.
Telemedicine involves the use of various technologies to transmit medical information from one location to another via electronic communications.These technologies, which are closely related to telemedicine services, include video conferencing, store-and-forward transmission of static images, remote patient monitoring (RPM) of vital signs, and telephone consultations.. In this report, we assessed whether each state’s Medicaid policies allow for the coverage and/or reimbursement of telehealth services utilizing these technologies.
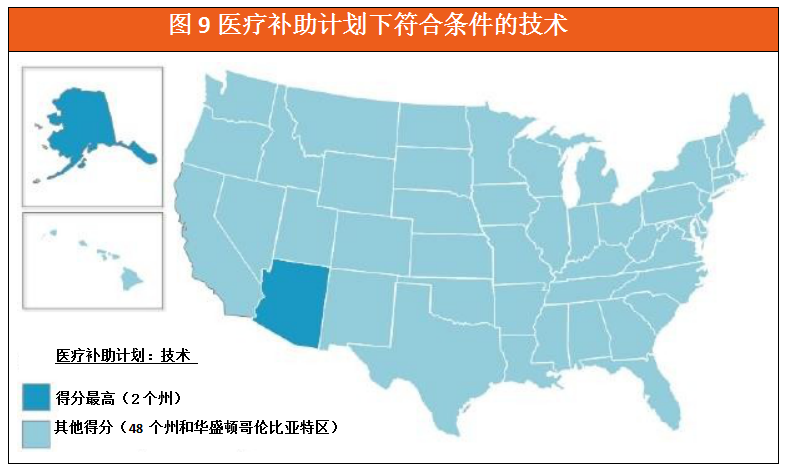
In the ranking for this indicator, 12 states scored above the average, with Alaska and Arizona achieving the highest scores (Figure 9). Alaska’s coverage of technologies includes interactive audio-video, store-and-forward, and remote patient monitoring used by telehealth providers, as well as audio-only conferencing encountered when providing certain telehealth services. Arizona permits various technologies, including telephone, video, and store-and-forward, to enable the delivery of remote patient monitoring services. Alaska, Arizona, Hawaii, Minnesota, Mississippi, Nebraska, Texas, and Washington all provide varying degrees of coverage for telehealth services utilizing synchronous technology, store-and-forward technology, and remote patient monitoring.VCBeat also found that fewer than 50% of U.S. states ranked low with failing grades (F), either because they only covered synchronous technologies or because they provided no coverage for telemedicine at all.
Furthermore, Idaho, Missouri, New York, North Carolina, and South Carolina prohibit the use of “mobile phone video” or “video calls” to deliver telemedicine services.
F. Distance or Geographic Limitations
In this report, distance restrictions are measured in miles and specify the minimum distance required between remote providers and patients to qualify for telehealth reimbursement. Geographic restrictions are defined as rural areas, urban areas, Metropolitan Statistical Areas (MSAs), specific population sizes, or Health Professional Shortage Areas (HPSAs).
We measured the distance or geographic conditions applicable to telehealth coverage and reimbursement under Medicaid policies.
Over the past year, states have made significant efforts to eliminate distance requirements in telemedicine services. States such as Hawaii, Idaho, and West Virginia now offer telemedicine services statewide. New Hampshire has enacted legislation that imposes geographic restrictions on telemedicine similar to those of Medicare. Indiana’s legislation has eliminated distance requirements for all telehealth providers but still enforces mandatory distance measures for certain eligible providers. Ohio’s Medicaid program has approved coverage for telemedicine services but has also opted to impose a five-mile restriction as a condition for reimbursement.
As shown in Figure 10,90% of states have not imposed distance or geographic restrictions on telemedicine. This finding dispels the misconception that telemedicine is only suitable for rural applications.。
This report assesses whether state Medicaid policies allow for the coverage and/or reimbursement of telehealth services provided by the following telehealth providers. The following are professionals who provide telehealth services:
• Physicians (MD and DO)
• Podiatrist
• Massage Therapist
• Optometrist
• Genetic Counselor
• Dentist
• Physician Assistant (PA)
• Nurse Practitioner (NP)
• Registered Nurse
• Licensed Nurse
• Certified Nurse-Midwife
• Clinical Nurse Specialist
• Psychologist
• Marriage and Family Therapist
• Clinical Social Worker (CSW)
• Clinical Advisor
• Behavior Analyst
• Substance Abuse/Addiction Specialist
• Clinical Therapist
• Pharmacist
• Physiotherapist
• Occupational Therapist
• Speech-Language Pathologists and Audiologists
• Registered Dietitian/Nutrition Expert
• Diabetes/Asthma/Nutrition Educator
• Home Medical Assistant
• Home Health Agency (HHA)
• FQHC
• CAH
• RHC
• CMHC
• SNF
Designated physicians receive 2 points, and designated other qualified providers receive 1 point. If the state imposes no restrictions on providers offering telehealth services, the maximum score of 35 points is awarded.
As shown in Figure 11, 19 states have not imposed specific restrictions on telehealth providers.
Other noteworthy trends include:
• Dental service coverage is expanding. Arizona, California, Colorado, Minnesota, Missouri, New York, and Washington have all extended coverage to include telehealth services provided by dentists.
• Alaska, California, Colorado, Illinois, Minnesota, Missouri, and Washington cover services provided by podiatrists. Alaska, California, and Kentucky cover services provided by massage therapists.
• Only California, Kentucky, Missouri, and Washington cover services provided by optometrists.
• Only Arizona, New Mexico, Oklahoma, and Washington cover services provided by behavior analysts in telehealth. This trend is noteworthy, as such specialists are critical to the treatment of autism.
• Other trends in behavioral health include that New Mexico, Oklahoma, Virginia, West Virginia, Wyoming, and the District of Columbia allow coverage for services provided by substance abuse or addiction specialists via telehealth.
Compared with previous reports, more states are expanding the categories of eligible providers to promote the adoption of telemedicine. Fourteen states rank low and receive a failing grade (F) because they authorize fewer than nine types of healthcare providers. Montana ranks last: its provider categories cover only physicians.
H. Telemedicine Services Provided by Physicians
Telemedicine services provided by physicians are generally covered and reimbursed by Medicaid programs. However, some plans impose specific health condition requirements for coverage, restrict the locations of patients and providers, limit the frequency of telemedicine use, or exclude services provided by other healthcare professionals.
In this report, we measured the restrictions imposed on healthcare professionals by telehealth coverage and reimbursement policies under Medicaid.
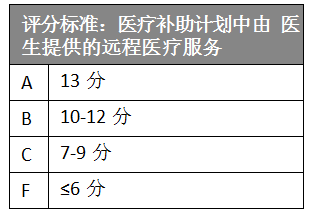
As shown in Figure 12, 13 states rank highly on this metric. These states do not impose scope-of-practice restrictions or additional requirements on services delivered via telehealth. Furthermore, these states permit physician assistants and/or advanced practice nurses to serve as qualified telehealth providers.Furthermore, most states cover outpatient services and counseling, while coverage for ultrasound and echocardiography is the lowest.
Connecticut, Florida, Hawaii, and Utah have been upgraded to an “A” rating, as they reformed relevant policies and lifted related restrictions, thereby expanding the coverage of telehealth services.
According to the American Telemedicine Association’s (ATA) guidelines for telemental health practice, telemental health services include remote interventions by mental health professionals using videoconferencing and other modalities. VCBeat has learned that means of delivering mental health services via telemedicine include, but are not limited to: mental health assessments, substance abuse treatment, psychological counseling, medication management, education, supervision, and collaboration. All states provide some form of telemental health services delivered via videoconferencing. Although the application of telemedicine in the field of mental health has increased across states, it is important to note that policies in this area vary significantly from state to state.
In this report, we measured the limitations of telehealth services in mental and behavioral health under Medicaid policies, as well as the types of providers permitted by each state to deliver services in this field.
Generally speaking,Telepsychiatry services commonly covered by Medicaid include mental health assessments, individualized therapy, psychiatric diagnostic evaluations, and medication management.As shown in Figure 13, 15 states rank highly in this area because none of them have imposed additional conditions on minimum service coverage or reimbursement for services delivered via telemedicine. Furthermore, these states have authorized at least one other category of healthcare professionals (such as physician assistants and advanced practice registered nurses) to serve as eligible telemedicine providers.
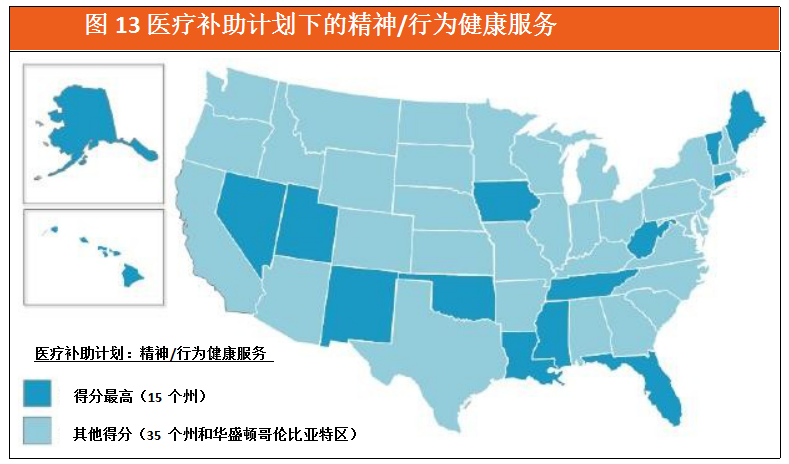
It is a relatively common practice across various states to allow psychiatrists, advanced practice nurses with clinical specialization credentials, and psychologists to provide tele-mental health services.services. However, many states also allow non-healthcare institutions to provide telemedicine services and receive reimbursement for them:
• Alaska, Arizona, Arkansas, California, DC, Delaware, Hawaii, Indiana, Kentucky, Michigan, Minnesota, Missouri, Nevada, New Hampshire, New Mexico, New York, North Carolina, Ohio, Oklahoma, Texas, Virginia, Washington, West Virginia, and Wyoming all cover telehealth services provided by licensed social workers.
• Alaska, Arizona, Arkansas, California, DC, Delaware, Indiana, Kentucky, Minnesota, Missouri, Nevada, New Mexico, Ohio, Oklahoma, Texas, Virginia, Washington, West Virginia, and Wyoming are all covered by telemedicine services provided by licensed professional consultants.
• Furthermore, only Arizona, New Mexico, Oklahoma, and Washington have mandated coverage for telehealth services provided by behavior analysts. This trend is noteworthy, as behavior analysts play a critical role in the treatment of autism.
New York State ranks lower with a grade of only C, as it imposes restrictions on technologies, vendors, and patient care settings for mental health services. Connecticut, Florida, Hawaii, and Utah have risen to an “A” rating by reforming relevant policies, removing existing restrictions, and expanding telehealth coverage in this field.
J. Rehabilitation Services
The ATA’s Telerehabilitation Guidelines define telerehabilitation as follows: “It is a service delivery model for rehabilitation that utilizes information and communication technologies. Clinically, this term encompasses monitoring, prevention, intervention, supervision, education, consultation, counseling, and other aspects of rehabilitation services.” Professionals involved in delivering rehabilitation services via telehealth technologies include neuropsychologists, speech-language pathologists, audiologists, occupational therapists, physical therapists, and others.
In this report, we examined the coverage and reimbursement of tele-rehabilitation services under Medicaid, as well as restrictions on service types, provider types, and patient or provider locations.
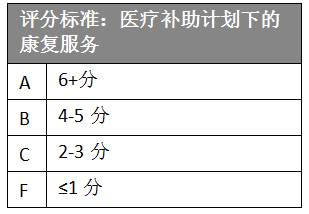
As shown in Figure 14, only 37 states are ranked on this indicator, because the Medicaid programs in the other 13 states do not cover rehabilitative services. State policies vary in scope and implementation; among them, 26 states already reimburse for telerehabilitation services under their Medicaid programs, with 14 of these states ranking highly.
Furthermore, among the 29 states where home health benefits cover telemedicine, only Alaska, Colorado, Florida, Hawaii, Iowa, Kentucky, Maine, Nebraska, Nevada, New Mexico, Tennessee, and Utah reimburse remote rehabilitation services under home health benefits.
One empirically validated form of telemedicine is remote patient monitoring, which encompasses continuous remote surveillance of vital signs or medication management provided by telehealth providers via video or audio, as well as physical measurements obtained through automated systems or telephone follow-ups.Remote monitoring methods for each patient should be tailored to meet the patient's needs and coordinate their care plan.
In home healthcare services, audio-video consultations can be utilized for skilled nursing, physical therapy, occupational therapy, or speech therapy outpatient care.
In this report, we examined the restrictions on provider types and service types for home healthcare services under the Medicaid program.
As shown in Figure 15, Hawaii and Utah have joined Alaska as the top three states ranking highest on this indicator.
Furthermore, among the 29 states that cover telehealth under home health benefits, only Alaska, Colorado, Florida, Hawaii, Iowa, Kentucky, Maine, Nebraska, Nevada, New Mexico, Tennessee, and Utah allow reimbursement for telerehabilitation services within home health care. Additionally, only Pennsylvania allows reimbursement for telehealth services provided by caregivers in the home.
The types of telehealth services covered under Arizona’s home healthcare benefits include live audio-video consultations, store-and-forward technologies, and remote patient monitoring. Seventy percent of states across the U.S. rank low in this metric and receive a failing grade (F), as their home healthcare benefits do not cover telehealth services.
In this report, we measured the restrictions on telemedicine applications under Medicaid and patient informed consent across states.
Among the 27 states with informed consent requirements, 18 states have mandates issued by their respective state medical boards (Figure 16). In Rhode Island and Connecticut, although both states’ Medicaid programs now cover telemedicine, their medical boards still require obtaining patients’ informed consent.
In this report, we assessed whether state Medicaid programs and medical board policies impose stricter requirements on telemedicine than on in-person consultations. State scores were determined based on whether the state mandates the presence of a telepresenter or healthcare provider.
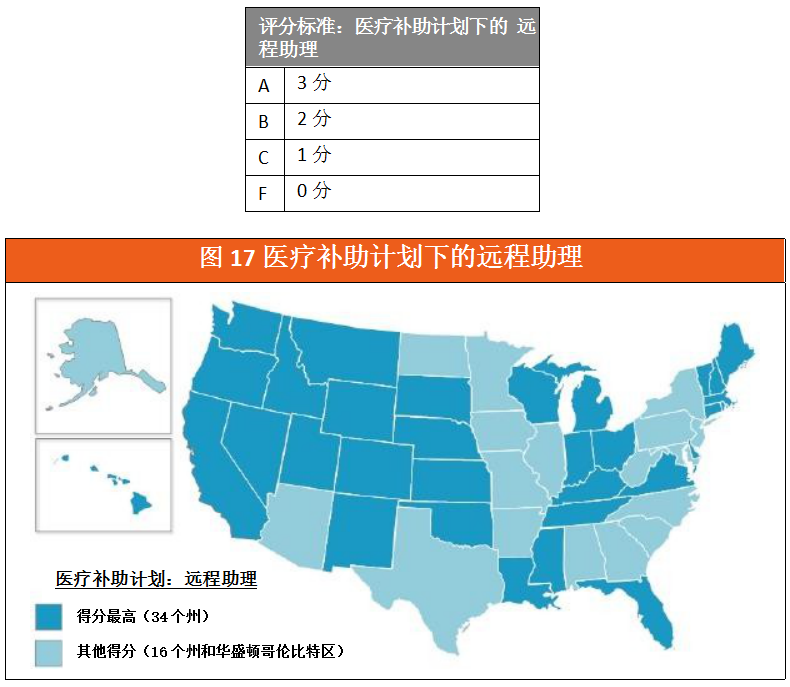
Alaska, Florida, and Oklahoma have raised their ratings to “A” due to policy reforms that eliminated many requirements for remote assistants. However, Alabama, Georgia, Iowa, Maryland, Minnesota, Missouri, New Jersey, North Carolina, and West Virginia only require that healthcare providers not be in the same location as patients during telemedicine consultations (Figure 17). New York requires the presence of a remote assistant during psychiatric telehealth services.
(3) Innovative Payment or Service Delivery Models
This report also includes records of innovative payment and service delivery models across various states. In addition to the networks established by each state in specialized nursing and correctional healthcare,The report also includes information on how various states have leveraged federal funding and waiver programs to improve access to and utilization of telehealth services.。
For many years,An increasing number of states across the United States are adopting Managed Care Organizations (MCOs) to establish capitated payment and delivery models, aiming to provide patients with better healthcare and follow-up services while controlling medical costs.. Such payment methods and operational details are diverse, offering valuable insights for establishing designated long-term healthcare delivery models. Managed Care Organizations (MCOs) that continuously experiment with innovative delivery models have also incorporated telemedicine into their coverage, as it helps reduce emergency department utilization and hospitalization costs.
Twenty-four states have already covered telemedicine under their Medicaid programs. Notably, Massachusetts and New Hampshire offer specified Medicaid coverage, but not under the fee-for-service (FFS) model.
The federal Affordable Care Act (ACA) provides states with funding and flexibility to expand their Medicaid programs and integrate dual-eligible beneficiaries (“dual eligibles”) enrolled in both Medicare and Medicaid. States such as Michigan, New York, and Virginia have expanded telehealth coverage and dual-eligibility enrollment among their populations through the Centers for Medicare & Medicaid Services (CMS).
The ACA also provides the Healthy Families Program to better coordinate primary, acute, behavioral, chronic disease, and social service needs across diverse populations. Chronic conditions include mental health disorders, substance use disorders, asthma, diabetes, heart disease, overweight (BMI > 25), and other conditions designated by CMS.
Nineteen states have approved the Centers for Medicare & Medicaid Services (CMS) Health Home Program amendments. Alabama, Iowa, Maine, New York, Ohio, and West Virginia have incorporated some form of telemedicine services into their approved Health Home Programs.
Medicaid programs include several options that cover remote patient monitoring, typically implemented through federal waivers. States can apply for such waivers to provide home and community-based long-term care services. Kansas, Louisiana, and Pennsylvania have utilized these waivers to offer home-based telehealth services to beneficiaries, particularly remote patient monitoring.