Professor Taosheng Huang of Cincinnati Children's Hospital Files IPO Prospectus Highlighting Mitochondrial Disease Research and 'Three-Parent Baby' Innovation
Source: GeneInsight PPT
Scientists, clinical experts, investment professionals, and corporate representatives are welcome to register for “Daka Lunjian.” Contact email: info@genonet.cn.
[Previous Reviews]
Season 2, Episode 1: Professor Huang Shangzhi
Season 2, Episode 02: Dr. Gu Weihong
Season 2, Episode 3: Professor Yao Hong
Season 2, Episode 4: Professor Zhao Haitao
Season 2, Episode 5: Vice President Wang Yi
Season 2, Episode 6: Professor Qi Ming
Season 2, Episode 7: Dr. Wang Wei
Season 2, Episode 8: Professor Ding Jie
Season 2, Episode 9: Dr. Dai Junbiao
Season 2, Episode 10: Dr. Shen Yue
"Big Names on Health" Issue No. 23
[Editor's Note]A mother lost all four of her children shortly after birth, likely due to genetic mutations in her mitochondrial DNA. She sought consultation with Dr. Zhang, a clinical geneticist, who identified a healthy female donor for egg donation. In this procedure, the nucleus of the donor’s egg was removed and replaced with the nuclear genetic material from the child’s parents. The resulting baby carries nuclear DNA from both parents and mitochondrial DNA from the donor female, thus becoming a “three-parent baby.” On April 6, 2016, the world’s first “three-parent baby” was born in New York (Reference 1). Today, we are honored to have Professor Huang Taosheng, a key member of the team behind the world’s first “three-parent baby,” share his research findings and experience on mitochondrial genetic disorders and three-parent babies. Professor Huang studied in the United States in the 1980s and has extensive expertise in clinical and molecular genetics. He has served as a frontline physician at Georgetown University Medical Center, Harvard Medical School, and Boston Children’s Hospital, and later as Director of Diagnostic Laboratories at the University of California, Irvine, and Cincinnati Children’s Hospital Medical Center. With rich theoretical and practical experience, he has actively engaged in academic exchanges between China and the United States. We sincerely thank him for accepting this exclusive interview with GeneInsight despite his busy schedule.

Three-Parent Babies and Mitochondrial Disease
Author: Professor Huang Taosheng
Director, Molecular Diagnostics Laboratory, Cincinnati Children's Hospital
Director, Center for Mitochondrial Diseases
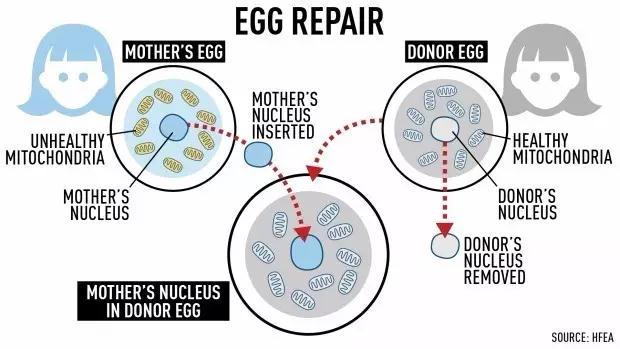
“Three-Parent Baby” Technology Schematic (Source: http://www.cbc.ca/)
GeneWisdom:Dear Dr. Huang,Thank you for accepting this exclusive interview with GeneInsight. You obtained your American Board of Pediatrics certification in 1996. From 1996 to 1999, you completed specialized training in clinical genetics and clinical molecular genetics at Harvard Medical School, passed the certification examinations administered by the American Board of Medical Genetics and Genomics (ABMG), and earned dual board certifications in Clinical Genetics and Clinical Molecular Genetics. During this period, you also served as an attending physician at Boston Children’s Hospital. Later, you moved from Harvard Medical School to the University of California, Irvine, where you served as a laboratory director. Currently at Cincinnati Children’s Hospital Medical Center, you have dedicated the past two decades to congenital heart disease, pharmacogenomics, and mitochondrial disorders. As a clinician-scientist who integrates roles as a specialist, director of a genetic diagnostic laboratory, and translational researcher, could you please provide a lay-friendly introduction to your research areas and highlight some of your milestone achievements for our readers at GeneInsight?
Prof. Huang: Thank you, Mr. Wang, for giving me the opportunity to conduct this interview. My current primary research focus is on mitochondrial genetics, a subfield of genetics dedicated primarily to the discovery of novel pathogenic genes. Broadly defined, mitochondrial diseases involve not only mitochondrial genes encoded by the mitochondrial genome but also numerous nuclear genes. Approximately 1,500 genes are involved in mitochondrial structure and function, and many additional pathogenic genes remain to be identified. As a specialist physician and director of a molecular diagnostics laboratory who also engages in basic research, my advantage lies in my ability to integrate clinical patient care, genetic diagnosis, and scientific research. This integration was the primary reason I joined this institution. Currently, my main research directions include three areas:
1) Discovery of new mitochondria-related pathogenic genes;
2) How to translate and apply findings from rare disease research to common diseases;
3) Alternative treatments for mitochondrial diseases.
GeneHub:You have been actively engaged in exchange initiatives between China and the United States, serving as a visiting professor or guiding expert at several domestic institutions, including Peking University, Zhejiang University, Peking Union Medical College, and the China Association for Healthy Birth and Child Care. You yourself hold ABMGG certification in clinical genetics and clinical molecular genetics, as well as medical licenses in two U.S. states. Based on your experience in cooperation and exchanges between China and the United States, what do you see as the primary differences between the two regions in the field of precision medicine? What strengths should peers and policymakers in both countries learn from each other?
Professor Huang: In the fields of precision medicine and medical genetics, there is a significant gap between China and Western countries. Medical genetics and precision medicine constitute a systematic engineering endeavor, particularly in the realm of rare diseases. Research on these conditions in Western nations typically originates from the clinical side, built upon long-term accumulation and a comprehensive system. In medical genetics, specialists first evaluate corresponding patients to characterize and define the disease, then select appropriate genetic tests based on clinical manifestations. Other areas, such as molecular diagnostics and cytogenetics, are established on this foundation. In the United States, genetic counselors are trained from among qualified physicians with clinical experience, and laboratory personnel—including those in molecular diagnostics, cytogenetics, and biochemistry—similarly possess robust clinical backgrounds. Consequently, medical genetics in the U.S. is segmented into several distinct components: medical geneticists, molecular geneticists, cytogeneticists, biochemical geneticists, and finally, genetic counselors. This highly specialized structural division differs markedly from the approach in China.
In China, medical genetics has not yet been established as a formal discipline. However, with national economic growth and the advancement of new technologies, genetic diagnosis has become highly active, and foreign technologies—such as sequence analysis tools—are being rapidly introduced into the country. Although there is limited original innovation, the speed of technology adoption is very fast. This rapid influx has led to significant challenges: physicians lack a solid foundational training, there is a shortage of true specialists in medical genetics, and there are insufficient specialist faculty to train professionals, including laboratory personnel and genetic counselors. Therefore, we advocate for the prompt development of medical genetics as a specialized foundational profession, which will in turn drive comprehensive training in genetics, encompassing laboratory practices and other related fields.
GeneHui:As a mitochondrial disease expert who has received major grants from the U.S. National Institutes of Health, could you discuss the characteristics of mitochondrial diseases, their impact on health and fertility, and how current precision medicine technologies are being applied to these conditions, drawing on one or two clinical cases? Given that mitochondrial diseases are relatively unfamiliar to most readers, your insights would be greatly appreciated.
Professor Huang: Regarding mitochondrial diseases, it is essential to first understand mitochondria. Mitochondria are involved in many major cellular functions, with energy metabolism being the most critical. The food we consume is converted into adenosine triphosphate (ATP), the energy required by the body, within the mitochondria. Since 90% of ATP is produced in the mitochondria, mitochondrial dysfunction can affect various organ systems throughout the body. In addition, mitochondria participate in many other vital processes, such as apoptosis. Therefore, mitochondria are closely linked to tumors, cardiovascular diseases, neurodegenerative disorders, and diabetes. Aging, a key area of current research, is also intimately associated with mitochondrial function. The term “mitochondrial diseases” commonly refers to relatively rare conditions, such as MELAS (Mitochondrial Encephalomyopathy, Lactic Acidosis, and Stroke-like episodes) or MERRF (Myoclonic Epilepsy with Ragged Red Fibers). These disorders result from mitochondrial dysfunction that impacts the nervous system and multiple organ systems. For instance, mutations in mitochondrial genes can cause sensorineural hearing loss and optic atrophy leading to vision impairment.
Currently, precision medicine plays a crucial role in the diagnosis and treatment of mitochondrial diseases. In the past, mitochondrial diseases were arguably the most complex disorders because they can affect any organ system, making clinical diagnosis highly challenging. Historically, in addition to routine examinations, muscle biopsies were commonly performed. Muscle biopsy is an invasive procedure that requires a series of subsequent tests. With the advent of precision medicine, genetic diagnostics have advanced rapidly. It is now possible to detect mutations not only in the mitochondrial DNA (mtDNA) but also across the entire nuclear genome, significantly improving diagnostic rates. For clinically typical cases of mitochondrial disease, approximately 50% can ultimately receive a definitive diagnosis. Nuclear gene mutations may follow autosomal dominant or recessive inheritance, X-linked dominant or recessive inheritance, or Y-linked inheritance patterns, whereas mutations in the mitochondrial genome are exclusively maternally inherited.
Shifting our research focus from mechanistic studies to clinical therapeutics is also part of our strategic direction. Below, I will discuss three-parent babies, or what we refer to as mitochondrial replacement therapy (MRT). Overall, the field of mitochondrial research is highly active. Mitochondria are not only implicated in most primary mitochondrial diseases but also associated with many common conditions, including cancer. Although oncogenic mutations may be present at birth, disease onset often occurs later in life. One hypothesis suggests that this delay is due to the accumulation of mitochondrial mutations and the progressive decline in mitochondrial function with aging. Many neurodegenerative disorders follow a similar pattern; for instance, Parkinson’s disease is closely linked to mitochondrial dysfunction caused by mutations in genes such as PINK1 and PARKIN, whose protein products function within mitochondria. As the central hub of cellular metabolism, mitochondria are also intimately involved in the pathogenesis of diabetes.
Over the past three to four years, our laboratory has identified five novel pathogenic genes associated with mitochondria. Although the population affected by any single rare mitochondrial disease is relatively small, the aggregate prevalence of these conditions appears comparatively higher when all causative genes are considered together. Nevertheless, mitochondrial diseases remain less common than other conditions, such as tumors. Consequently, another focus of our current research is to translate findings and achievements from rare disease studies into applications for more common conditions. For instance, given the significant role of mitochondria in aging—a universal human experience—our recent research direction centers on investigating aging from a mitochondrial perspective.
GenePlus:In April 2016, the world’s first “three-parent baby” was born in New York, USA. This male infant carries genetic material from three individuals: a Middle Eastern couple and a healthy female donor who provided mitochondria. The mitochondrial replacement therapy was performed in Mexico, while the child was delivered in New York. As a key participant who completed this study together with Dr. John Zhang, could you share with scholars in China the full story behind the “three-parent baby,” as well as the technological, reproductive, and ethical implications of this innovative achievement?
Prof. Huang: The three-parent baby born last year came from a large family in which many members had died from this disease. The mother had experienced four miscarriages, and her two children passed away at 5 months and 15 months of age, respectively. She had no living children when she sought medical consultation. This is not an isolated case; in fact, there are many similar families, including numerous ones in China. At that time, we developed a treatment plan for her using nuclear transfer technology. Our collaboration with Dr. Zhang Jin was highly successful; the child is now nearly 11 months old, in excellent health, and free of any issues. The procedure was performed in Mexico, as it was not yet legally permitted in the United States. We had intended to carry this out four years ago, having anticipated that U.S. approval would be granted soon.
The U.S. National Academy of Medicine has stated that this represents a highly significant breakthrough—ranked fourth in *Science* and eighth in *Nature* among last year’s top news stories—and emphasized its critical importance for implementation. This technology also holds broad potential for other applications. Although the UK Parliament passed legislation approving this approach some time ago, it remained unimplemented until recently. Following the birth of our “three-parent baby,” we have maintained regular communication with relevant UK government agencies. The UK government has now granted formal approval, making the United Kingdom the only country where three-parent baby treatment is legally permitted. In contrast, many other countries worldwide lack clear legal regulations on this matter (see Reference 2).
We hope that with technological advancements, this technology can be widely adopted. Given that the primary contributors to this field are Chinese, I hope China can leverage its proximity and advantage, with the government easing relevant regulations to accelerate its application. Many people may not fully understand this, but witnessing the suffering of these families brings profound empathy. As a specialist physician, I encounter such families daily, and I am eager to provide them with this therapeutic technology, helping them achieve happy and fulfilling family lives.
GeneHui: You initiated clinical trials for congenital heart defects as early as 2007 and have also conducted some exploratory work in pharmacogenomics. The integration of clinical molecular genetics with modern technologies such as gene sequencing and microarrays has significantly advanced the field toward precision medicine, greatly improving diagnostic capabilities. What are the current major challenges in therapeutic development, particularly in pharmacogenomics? Some pharmaceutical industry peers have reported that the top-level design of precision medicine data does not meet the standards required for new drug development. Are there other factors involved? Furthermore, how should we promote the application of genomic big data to advance pharmacogenomic research? Thank you!
Prof. Huang: I previously served as the Director of the Department of Cardiovascular Genetics for an extended period. Congenital heart disease remains highly prevalent, with the majority of our work focused on clinical practice, while research efforts have primarily centered on genetics. Prevention of cardiovascular diseases, particularly congenital heart disease, is quite challenging; however, given that it is the most common congenital defect, this issue warrants significant attention.
The U.S. Food and Drug Administration (FDA) maintains a dedicated website on pharmacogenomics (Editor’s note: see Reference 3 at the end of this article). Its clinical application is highly routine and systematic. The FDA mandates genetic testing prior to the use of many medications, which constitutes an integral part of precision medicine. Given that individuals may exhibit varying responses to drugs, including differences in drug metabolism and intracellular reactions, pre-treatment genetic screening is crucial in many cases. This approach helps optimize therapeutic efficacy and minimize adverse effects, as certain medications may be beneficial for some patients but ineffective or even harmful to others.
References and Literature:
1. http://www.cbc.ca/news/health/3-parent-baby-birth-1.3781026
2. http://www.bbc.com/news/health-31594856
3. https://www.fda.gov/drugs/scienceresearch/researchareas/pharmacogenetics/ucm083378.htm