World's First Robot-Led Cochlear Implant Surgery Successfully Completed: Surgeons Witness a Paradigm Shift in Microsurgery
Recently, the website of *Science Robotics* published an article stating that researchers at the University of Bern have developed a robot that assisted physicians in successfully performing a cochlear implant surgery. This procedure differs from previous surgeries performed using robotic systems such as the da Vinci Surgical System:In procedures where the surgeon operates the robotic arms, this robot performs surgeries under physician supervision, with the robot serving as the primary surgeon.
VCBeat has learned that, compared with humans, surgical robotic systems outperform humans in terms of perception, dexterity, and procedural scale, making them inherently well-suited for surgical procedures. Furthermore, although the scientific community has conducted in-depth research,Image-Guided Robotic TechnologyThe number of clinical cases involving its application in microsurgery remains limited.
Among these, the greatest challenges are geometric scale and tactile resolution. At such scales and resolutions, surgeons cannot adequately control devices that operate beyond the limits of human capability. For safety considerations, physicians must perform numerous complex operations, much like pilots interacting with instrument panels in avionics systems.
Cochlear implantation is a microsurgical procedure that requires submillimeter precision and a reliable visual feedback system. Robotic cochlear implantation systems can enhance the consistency of surgical outcomes, such as preserving residual hearing and reducing surgical invasiveness.
Robot-Assisted Minimally Invasive Surgery
Approved by the Bern Ethics Committee in Switzerland and national medical device regulatory authorities, researchers conducted a clinical trial in the summer of 2016, selecting a 51-year-old female patient with bilateral deafness for unilateral cochlear implantation in the right ear. Postoperative CT imaging was used to verify the geometric accuracy of the drilled tunnel, and pre- and postoperative levels of facial nerve activity and taste function were measured and compared to determine the effectiveness of the safety mechanisms employed, yielding promising results.
Traditional surgical robots assist physicians in performing surgeries, whereas the robot designed this time performs surgeries autonomously. Let us first examine the flowchart:
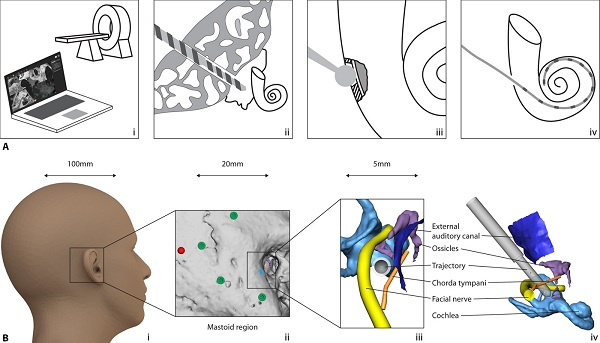
First, a hole is drilled behind the ear, then the electrode array is inserted. Next, an opening is made in the cochlea of the inner ear to insert the artificial cochlear implant, completing the procedure. It is important to note the operational space required by the robotic system: while it ranges from 100 millimeters down to 5 millimeters, the robot can still drill holes for millimeter-scale electrodes within a confined 5-millimeter space—a task that is extremely difficult for conventional surgeons to perform.
The traditional surgical procedure typically involves making a large incision behind the ear, reflecting the skin flap posteriorly, excising certain tissues, drilling a bone bed in the skull, and then implanting the cochlear implant.This can cause permanent damage, whereas robotic surgery is minimally invasive.
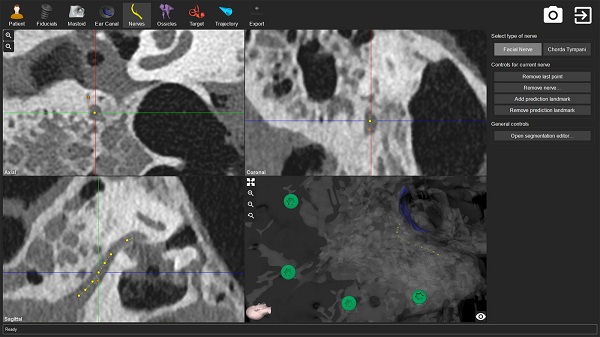
The reason surgeons are confident in having robots perform this surgery is that the robot possesses two key capabilities: “surgical planning intervention” and “postural assessment of drilling force and bone density.” Researchers state that prior to using the robot for surgery, surgical planning intervention is conducted. The planning software tools allow for general image segmentation (identification of reference screws, shown in green), segmentation of anatomical structures (facial nerves, shown in yellow), and parametric configuration of general treatment plans.
Meanwhile, the optimal trajectory pose is calculated by leveraging the correlation between bone mineral density (derived from CT) and drill bit force (recorded during the drilling process).
Furthermore, during the manual optimization of the trajectory orientation, the software automatically calculates the geometric distance from the trajectory to the surrounding modeled anatomical structures, as well as the angle between the trajectory and the path of the basal turn of the cochlea, to facilitate optimal insertion of the implantable electrode. During the registration step, the software detects the fiducial screws placed in the lateral skull base of the patient for surgical documentation. To meet precision requirements, researchers employed a fiducial volume accuracy and image-matching variation model to automate and validate the detection of fiducial screws. Comprehensive general image quality tests were implemented to detect unacceptable image artifacts or insufficient image contrast levels.
Levels of Robotic Automation
Science Robotics also published an article proposing a classification system for robots based on their level of automation, ranging from Level 0 (teleoperated robots) to Level 5 (fully autonomous robots capable of performing surgeries independently). Although there have been numerous challenges in the application of robotics in natural medicine, and achieving Level 5 remains somewhat distant, it is still necessary to plan ahead.
If dreams were to become reality, and if system classification reached Level 4 or Level 5, this robot would no longer be merely a medical device; it would replace physicians and effectively practice medicine autonomously. At that point, how should laws, regulations, and ethics be adjusted? VCBeat believes that raising such questions for consideration is certainly not wrong.
Meanwhile, robots have taken on a significant portion of physicians’ workload. Although they will not replace doctors, will the training, education, and income of physicians change accordingly?