Global Home Healthcare Nursing Market to Reach $349.8 Billion: China's Market Remains Underdeveloped
By Luo Mei and Liu Lushi
Home nursing services have never been fully liberalized in China. The term “home nursing” referred to here denotes a model whereby patients requiring intravenous infusion can receive immediate in-home service from a nurse upon making a phone call; the primary role of these “home-visit nurses” is to provide intravenous infusion therapy at patients’ homes.
Abroad, however, "home visit nursing" services are commonplace.
So, what are the obstacles hindering the development of domestic “home-visit nursing” services? What lessons can be drawn from overseas home-visit nursing models? How should emergency medical issues encountered during home visits be handled? What is the market size for home-visit nursing? And how can profitability be achieved? …
With these questions in mind, VCBeat (WeChat: vcbeat) hopes to lift the veil on home-visit nursing services through this report and highlight some leading companies already operating in this field.
Tracing the History of Overseas “Home-Visit Nurses” Providing Medical Services,As early as 1893, Lillian Wald, a pioneer of public health in the United States, firmly believed that public health nurses should not merely care for patients but also address broader social issues. Together with Mary Brewster, she co-founded the Henry Street Settlement, a non-profit organization providing medical care to the impoverished. One of its divisions was called the “Visiting Nurse Service,” which marked the genesis of home-based nursing care. In 1944, this division separated from the Henry Street Settlement and became the “Visiting Nurse Service of New York (VNSNY)", today, it has becomeThe Largest Nonprofit Home and Community-Based Healthcare Organization in the United States。
Now, in addition to the largest visiting nurse organization in New York, states such as Iowa, Maine, and New Jersey have their own visiting nurse organizations. Visiting nurses have a national professional association, calledVisiting Nurse Association of America(VNAA), representing more than 150 home health and hospice agencies from over 40 states across the United States. These agencies may be operated by private enterprises, non-profit organizations, faith-based organizations, or government entities, and may function independently or as affiliates of healthcare institutions. There is also a non-profit organization in the United States calledChina Home Healthcare and Hospice Care Association, representing more than 33,000 home health care agencies across the United States, as well as over 2 million nurses, caregivers, physical therapists, and other professionals.
In Japan, a country with severe population aging, the development model of home-based medical care is also highly representative. Since the 1970s, Japan has been developing various forms of home care services. In 2000, Japan introduced Long-Term Care Insurance, integrating medical care with long-term care, and gradually formingStandardized "Home-Based Medical Care" Services. Here, every individual requiring home-based medical care is supported by a comprehensive healthcare team, including physicians, nurses, dentists, pharmacists, physical therapists, speech-language pathologists, and personal care attendants, among others.
Markets & Markets, the world’s second-largest market research and consulting firm, previously projected that the global home healthcare market would reach a total value of $349.8 billion by 2020. According to its statistics, the market was valued at $227.5 billion in 2015, with an expected compound annual growth rate (CAGR) of 9% through 2020.
The home healthcare market in the United States has gradually matured, capturing a significant market share. Here, VCBeat outlines the operational performance of several of the largest home healthcare companies in the U.S. According to the latest rankings of U.S. home health agencies by LexisNexis, the top five institutions by national market share are Kindred Healthcare, Amedisys, LHC Group, Almost Family, and Encompass Home Health. The total revenues for these companies in 2016 were as follows: Kindred Healthcare reported $7.2 billion, a year-on-year increase of 2.3%; Amedisys reported $1.437 billion, a year-on-year increase of 12.3%; LHC Group reported $915 million, a year-on-year increase of 12.1%; and Almost Family reported $623 million.
Behind the profitability of these institutions lies high-quality service offerings.
In the United States, home healthcare organizations typically involve two categories of service providers:Registered Nurse (Registered Nurses), Health Aides。
01
Registered Nurse.
During home healthcare visits, medical procedures are performed in accordance with physicians' orders. Specific job responsibilities include:
· Infusion, Injection, specialized wound care, urinary catheterization, colostomy care, etc.;
· Follow the dosage and scheduled times as prescribedDrug Administration Therapy, including oral and intravenous administration;
· Various immunizations, fertility-related injections (such as in vitro fertilization), etc.;
· 24/7 postoperative observation and nursing care;
· Assess home safety.
02
Health Caregiver.
During home visits, their primary services include companionship and caregiving, with the responsibility of notifying nurses in case of emergencies. Specific job duties include, but are not limited to:
· Medication reminder.
· Record vital signs such as pulse and blood pressure;
· Provide personal care assistance, such as bathing and dressing;
· Short-term care following injury or surgery;
· Provide long-term care for individuals requiring extended supervision, such as those with Alzheimer's disease.
In Australia, home-visit nurses will be able to provide in-home services such as wound dressing, asthma testing, and vaccine administration. They also conduct patient education, imparting knowledge on the management of chronic conditions like diabetes and heart disease to deliver long-term benefits. Additionally, nurses are responsible for performing Pap smears, blood glucose tests, and cholesterol tests, as well as coordinating with specialists for treatment and follow-up care.
In Sweden, specialized diabetes nurses provide home care services, dispatched from outpatient clinics at community hospitals. These nurses educate newly diagnosed patients about diabetes, distribute educational materials, instruct them on the use of blood glucose meters, schedule regular monitoring of blood glucose and blood pressure, and arrange follow-up visits, including coordinating with physicians to conduct fundus examinations within the community.
In terms of payment,The United States isThe First in HistoryCountries Combining Insurance with In-Home Medical Care CostsIn 1909, the Henry Street Settlement partnered with Metropolitan Life Insurance Company to include home nursing costs in users' health insurance policies. Today, the United States has incorporated home healthcare costs intoMedicare (Medicare), covered expenses include short-term skilled nursing care, physical therapy, and speech therapy, while costs for 24-hour home care, shopping, cleaning, and assistance with bathing and dressing provided by caregivers are not covered by insurance.
In Japan, home-based medical care is also integrated with health insurance., in which physician visits and some nursing visits are conducted byMedical Insurancecoverage, while other services are provided byLong-Term Care Insuranceburden. Thanks to its comprehensive health insurance system, in-home medical services have become affordable.
Take the U.S. home healthcare system, for example; it is relatively mature. In the United States, registered nurses who provide home care are highly skilled professionals with experience in both hospital and home settings. Their nursing licenses are issued by state boards of nursing. They typically hold an associate degree in nursing from a community college or have completed a four-year bachelor’s degree program. After entering the workforce, nurses also undergo regular training to continually refine their clinical skills.
When it comes to the management of registered nurses by home healthcare agencies, it is necessary to discuss the U.S. healthcare system, which differs significantly from that of China. In the United States, healthcare professionals maintain a relatively independent relationship with hospitals: physicians and nurses may be employees of hospitals or healthcare organizations; they may also join professional medical groups to work for multiple contracted hospitals; or they may practice in community clinics. Therefore, the practice of “multi-site practice” among healthcare professionals is quite common.Medical safety issues are largely covered by medical liability insurance.. The United States offers various types of medical professional liability insurance tailored to different categories of healthcare providers, such as physicians, nurses, and even medical service volunteers. Similar to the coverage provided for nurses working in hospitals, nurse liability insurance also extends to home-visit nursing services.
Home healthcare agencies all emphasize in nurses’ job responsibilities that, compared with hospitals, the home setting poses higher risks during emergencies, and nurses must carry out home-based care in strict accordance with physicians’ orders.
However, the well-trained nursing workforce in the United States has long sought greater responsibility and autonomy, rather than merely following physicians’ orders. Linda Aiken, Director of the Center for Health Outcomes and Policy Research, stated, “Hundreds of studies have shown that the care provided by nurse practitioners sometimes surpasses that provided by physicians.” In 2016, Florida, the last U.S. state to do so, granted prescriptive authority to nurses.The Expansion of Power Among Nurse Practitioners Is an Undeniable Trend, and their confidence in shouldering this heavier responsibility is underpinned by stringent professional ethical standards and a rigorous, continuous education and training mechanism.
In the United States, home health aides providing in-home care are trained and licensed by state departments of health. Home health aides employed by home healthcare agencies undergo rigorous background checks, screening, and management, primarily reflected in the following aspects:
1. Before caregivers commence their duties, the agency conducts thorough background checks to ensure the safety of service recipients. The details of the investigation are as follows:
· Family Health Nursing Competency Examination Score;
· In-depth personal interviews;
· Verify the valid status of registration certificates from the National Caregiver Nurse Registry;
· Past work records;
· At least a national-level criminal background check;
· Conduct health screenings in accordance with institutional policies or state laws;
· Verify that the applicant possesses: a compassionate attitude when caring for patients; the maturity and competence required to perform duties effectively; the ability to read, write, and carry out healthcare activities as instructed; and proof of successful completion of a home health aide training program in accordance with legal requirements and state and federal regulations.
2. During the care process, to ensure that caregivers have provided care to users, supervision methods include:
· View time logs and attendance records;
· View home care worker visit documentation;
· Monitor patient complaints;
· Investigate patient satisfaction;
· Monitor whether the in-service education received by caregivers meets the required duration.
On the basis of the aforementioned regulatory oversight of nurses and nursing assistants, the primary solution adopted by these home-based medical care institutions to address negligence and accidents in home healthcare remainsPromptly provide reassurance to the patient and their family, and negotiate compensation.。
In the United States, home healthcare organizations (agencies that dispatch nurses and caregivers to provide non-acute, in-home care) have evolved over more than a century into a highly mature market with comprehensive regulatory frameworks.
Home health agencies, as regulated by the Centers for Medicare & Medicaid ServicesMust participate in the Medicare or Medicaid program.Part-time nurses must provide services under the supervision of professional full-time nurses; medical consumables and durable medical equipment must be available; if the institution is affiliated with a hospital, resident physicians may provide home-based medical care; if the equipment required for treatment is difficult to transport, home healthcare services are not supported.
Each state has its own distinct regulations regarding the safety of home healthcare. Common elements include: protecting care recipients from abuse and harm; providing sterile medical devices and needles; ensuring that healthcare providers are free from alcohol or drug abuse; and guaranteeing the proper use of medications and controlled substances.
There are also certain liability exemptions defined for nurses’ home-based medical services. For instance, the U.S. Department of Labor once provided an interpretation in a case involving home healthcare—specifically, home-based diabetes treatment,Nurses are not liable for unsafe medical supplies (e.g., syringes) provided by patients themselves.。
As China’s population aging deepens, the demand for elderly care and medical services continues to grow. The “integrated medical and elderly care” model is poised to become a breakthrough in ensuring that older adults in an aging China have access to both care and medical treatment. By the end of 2014, the number of people aged 60 and above in China had reached 212 million, accounting for 15% of the total population. Among them, a large proportion suffer from chronic diseases, and nearly 40 million are disabled or partially disabled. This has made the overlapping trend of demand for medical and health services and daily living assistance among the elderly increasingly evident.
"Integrated medical and elderly care is a new model of elderly care that combines medical services with senior living. Its advantage lies in integrating resources from both sectors to provide continuous care, while also improving hospital bed turnover rates. However, home-based elderly care better aligns with China's national conditions."
A crucial component of home-based elderly care is whether medical professionals can provide in-home medical services to the elderly. The National Health and Family Planning Commission stated that a preliminary policy framework and standardized guidelines for integrated medical and elderly care would be established by 2017.
In May 2016, the Guangdong Provincial Health and Family Planning Commission issued the "Key Work Plan for Continuously Improving Nursing Services in Guangdong Province," which explicitly supported exploring multi-site practice for nurses. The plan encouraged regions with appropriate conditions to pilot multi-site nursing practice; urged specialist nurses from tertiary hospitals to establish specialist nursing clinics at primary healthcare institutions; promoted nurses at hospitals above the county level to provide post-discharge transitional care and long-term care services through various models; supported primary healthcare institutions in delivering home-based nursing services; and encouraged nurses to conduct regular visits or work part-time at nursing homes and long-term care facilities. Once multi-site practice for nurses is fully implemented, it will mean that nurses can practice flexibly at multiple locations after registering in one jurisdiction. Furthermore, nurses practicing through online appointment platforms will have clear policy support.
In seven months, Beijing will implement six new favorable medical insurance policies, focusing on the implementation of tiered diagnosis and treatment and the integration of medical care with elderly care. Specific measures include expanding the scope of medications covered by basic-level medical insurance, increasing the reimbursement rate for outpatient visits at community clinics, enabling reimbursement for long-term prescriptions issued to patients with four types of chronic diseases, and incorporating home-based medical services and the establishment of home hospital beds into the medical insurance payment coverage.
According to the Beijing Municipal Human Resources and Social Security Bureau, Beijing will launch a pilot program for long-term care insurance for disabled elderly individuals starting next year. The program targets elderly insured persons who have been in a state of disability for an extended period, providing them with services necessary for daily basic personal care. Policy-relatedLong-Term Care InsuranceAs an insurance system with the nature of social insurance, it is mandatory.
Currently, Fengtai District in Beijing has launched preliminary pilot programs for home-based medical services in seven community health service centers, providing in-home medical care to elderly individuals who are unable or partially able to care for themselves, particularly those from advanced-age families and families facing family planning difficulties. Building on the pilot program for home-based elderly care services in Fengtai District, Beijing will expand the scope of such pilots. The Beijing Municipal Health and Family Planning Commission disclosed that pilot programs have been confirmed in Dongcheng, Chaoyang, Haidian, and Fengtai districts, where community health service institutions will provide in-home services to elderly residents. Pilot plans have been formulated to actively encourage elderly individuals living at home to sign contracts with community health service teams, and to incentivize these institutions to offer services such as home visits, home hospital beds, and in-home rehabilitation and nursing care for elderly patients with serious illnesses, disabilities, partial disabilities, or other mobility limitations and genuine difficulties.
A survey article titled “Investigation and Analysis of Nurses’ Perceptions of Multi-Site Practice,” jointly published by the School of Nursing at Capital Medical University and the Nursing Department of Tiantan Hospital in the Chinese Journal of Nursing (January 2017 issue), showed that the majority of nurses welcome multi-site practice. Among the 1,010 nurses who participated in the survey, 78.5% supported nurses engaging in multi-site practice. Most nurses believed that multi-site practice could increase their economic income, enhance their self-worth, and improve their professional skills.
The Beijing Municipal Health and Family Planning Commission stated that the next step will be to develop the "Catalogue of Home-Based Services for the Elderly," starting with services in high demand among older adults, so as to gradually standardize home-based medical and nursing care items, service content, and operational protocols. Priority will be given to providing home hospital bed services for elderly individuals who are advanced in age, disabled, living alone (empty-nesters), or have limited mobility. These services will be delivered in accordance with the city’s established guidelines on types of home hospital beds, scope of admission, management requirements, and operational standards.
1. Policy on nurses practicing at multiple sites awaits liberalization.Although China has opened policy channels for physicians to practice at multiple sites, no policy relaxation has yet emerged for “nurses practicing at multiple sites.”
2. There should be entry requirements for registered nurses.Home visits by nurses are beneficial to patients, particularly those with limited mobility, and represent a future trend. It is also a promising direction for currently employed or retired nurses to provide home-based care services. Meanwhile, it is essential to emphasize that while patient needs can be met, potential risks must be regulated and mitigated in advance, and there should be established bases and channels for resolving any disputes or issues that may arise.
It is advisable to avoid selecting nurses who are young, have limited years of nursing experience, or lack sufficient practical expertise. Home-visit nurses should meet certain thresholds in terms of years of service and clinical experience.
4. Enhance nurses’ awareness and competence in emergency resuscitation during home visits.Nurses providing home-based care outside the hospital setting face numerous challenges, such as medication safety and allergic reactions.
5. The scope of nursing services provided by nurses during home visits must be clearly defined, and patients requesting such services must undergo an assessment.It is recommended to sign community home health service agreements and informed consent forms with the community health center nearest to the patient. Physicians or nurses must complete home visit assessment forms, initial consultation records, and other required documentation. It is mandatory to maintain records for every step and ensure that all procedures are fully documented and traceable.
6. Mitigate risks, such as medical risks, legal risks, and personal accident risks.To mitigate these risks, in addition to the home-visit nursing service platform itself ensuring the legality and compliance of the services provided, it should establish standardized processes and secure insurance coverage as a basic safeguard.
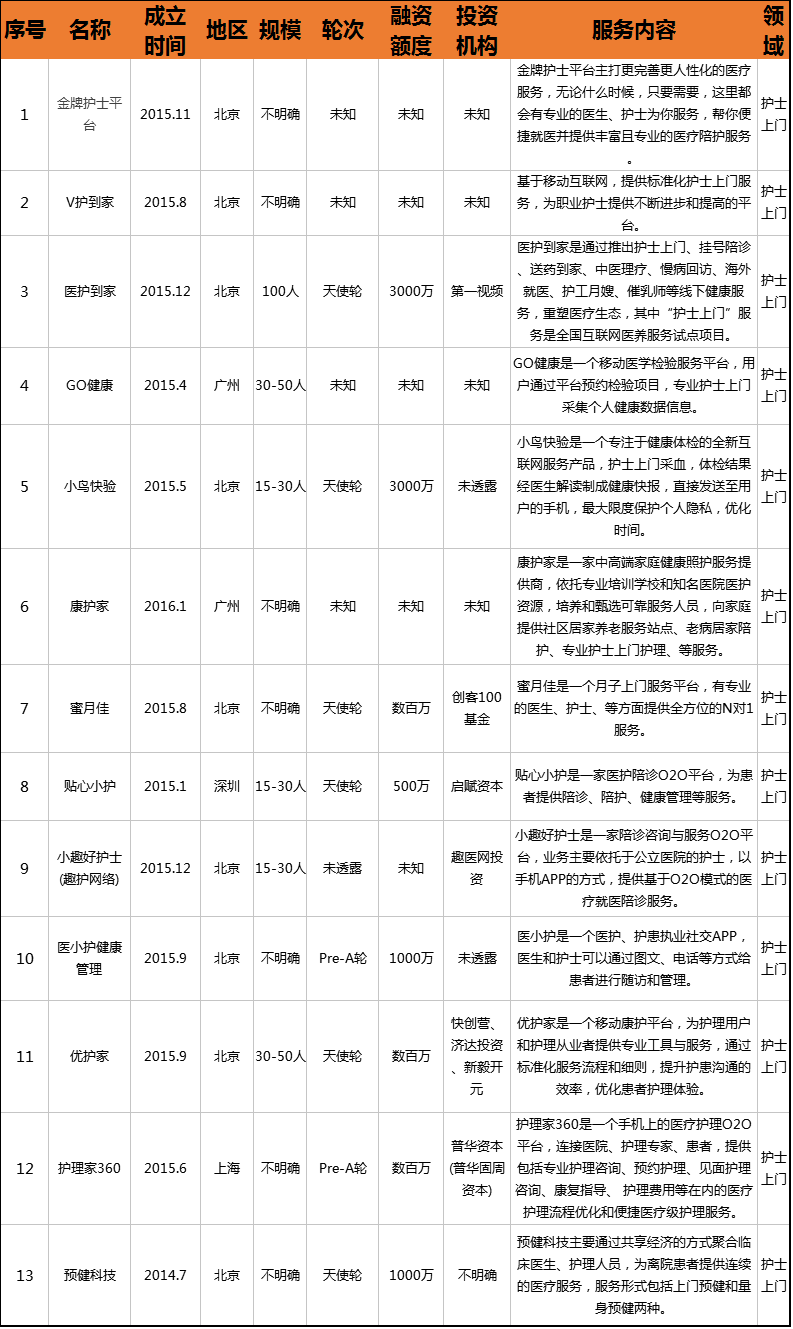
Among the 13 listed companies, few home-based nursing service projects have attracted capital investment. These companies are primarily concentrated in Beijing, Shanghai, Guangzhou, and Shenzhen, with nine in Beijing, two in Guangzhou, one in Shanghai, and the remaining two in Shenzhen.
From the perspective of market entry, approaches have targeted sectors such as maternal and infant care, women’s and children’s health, and elderly care, all of which involve home-visit nursing services.
It is evident that China’s market for home-visit nursing services holds immense potential, with a long road still ahead.
01
Kaiser Permanente's In-Home Healthcare Program — Primary Care @ Home
Kaiser Permanente launched the Primary Care @ Home program, establishing its unique model of in-home medical care in the U.S. Pacific Northwest (Oregon and Washington). In this program, “office-free” healthcare professionals deliver patient-centered care. The care team has since expanded to include nurse practitioners, physician assistants, clinical pharmacists, geriatric psychiatrists, and other specialists. In 2013, the Primary Care @ Home program partnered with Metro West Ambulance, enabling seamless integration between in-home care providers and emergency services.
Currently, Primary Care @ Home has over 1,300 members, and surveys indicate that the home-based medical care program can reduce patients’ total healthcare costs by 25%.
02
Kindred at Home
Kindred at Home is a subsidiary of Kindred Healthcare, a non-acute medical care company, and serves as its home healthcare division. In addition to basic disease management and wound care, it also provides services such as physical therapy, speech therapy, and occupational therapy.
Kindred’s home care services are specifically tailored for patients with heart disease, Alzheimer’s disease, Parkinson’s disease, rheumatism, stroke, chronic obstructive pulmonary disease (COPD), heart failure, and those recovering from orthopedic surgery. The team possesses extensive expertise in home-based medical management and the characteristics of complications associated with these conditions.
Kindred Healthcare, founded in 1968, boasts a robust healthcare network comprising hospitals, nursing centers, and partnerships with rehabilitation facilities across the United States, currently ranking first in the U.S. home healthcare market share. It has been named one of “America’s Most Admired Healthcare Companies” by Forbes for five consecutive years and ranked 410th on the Fortune 500 list in 2013. Kindred Healthcare went public in 2001.
03
Uber Delivers Nurses to Your Doorstep
In 2015, Uber launched its “Nurse On-Demand” service in 36 cities across the United States, enabling users to receive in-home influenza vaccination services. For just $10, a registered nurse would visit to administer flu vaccines to users and their family members or friends (up to a maximum of 10 individuals). The core focus of this service was to bring healthcare professionals—including physicians, nurses, and pharmacists—directly to patients.
As early as 2014, Dr. John S. Brownstein, Chief Expert at the Innovation Office of Boston Children’s Hospital and Associate Professor at Harvard Medical School, proposed this idea to Uber. Uber accepted the proposal and launched a home-based influenza vaccination service, with more than 2,000 residents in Boston, Chicago, New York, and Washington becoming the first beneficiaries of this initiative.