Cerebral Palsy Treatment Report: Cerebrolysin Boosts Social Skills by 65%, Five Cell-Based Therapies Show High Potential
Pediatric cerebral palsy, commonly known as cerebral palsy, refers to a group of clinical symptoms resulting from non-progressive brain injury during the immature stage of brain development within one month after birth.Its primary clinical manifestations are motor and postural dysfunction, often accompanied by speech, cognitive, auditory, and visual impairments, as well as epilepsy, secondary muscle contractures, and limb deformities. It is the most common cause of disability in children.。
The global prevalence of cerebral palsy (CP) in children is substantial, affecting 1 to 5 per 1,000 live births, with approximately 17 million people worldwide living with the condition. Various prenatal and postnatal factors can contribute to the development of CP, including hypoxia, trauma, infection, genetic factors, and developmental brain abnormalities.
Cerebral palsy can be classified into spastic, athetoid, rigid, ataxic, tremor, hypotonic, and mixed types. Studies have shown that three-quarters of children with cerebral palsy experience pain; half have intellectual disabilities; one-third are unable to walk; one-quarter are unable to speak; one-quarter have epilepsy; and one-tenth are blind. Thus, it is evident that cerebral palsy has a significant impact on individuals, the healthcare environment, and the socioeconomic landscape.
The history of efforts to combat cerebral palsy dates back to the 1840s. At that time, John Little, an orthopedic surgery specialist in the United Kingdom, pioneered research into cerebral palsy. Over the subsequent century, numerous treatment systems have been established and developed. In the second decade of the 21st century, with the rapid development and application of digital technologies, an increasing number of high-tech approaches for treating cerebral palsy have emerged. VCBeat (WeChat ID: vcbeat) has summarized the current conventional clinical treatments for cerebral palsy, as well as several of the latest digital solutions, to help you understand how technology is driving and supporting clinical medical practice.
Conventional treatment for cerebral palsy primarily focuses on symptom management. Currently,Healthcare institutions commonly adopt a combination of approaches, such as medical interventions, rehabilitation, surgery, orthotic devices, and botulinum toxin type A injections, to improve patient function.。
For a long time, it was widely believed that damage to the human central nervous system was irreversible. However, with the continuous advancement of medicine, the emergence of various nerve regeneration techniques has made repair of the central nervous system possible. These methodsIt mainly includes two major categories: neurodegenerative disease drugs and cell therapy.。
Pharmacotherapy
Oxiracetam is a central nervous system agent that selectively affects cortical and hippocampal neurons, facilitating functional recovery of nerve cells. It activates glutamate receptors in the human brain and modulates the actions of acetylcholine and glutamate. This enhances neuronal metabolic activity, thereby improving learning capacity, memory, and activities of daily living in patients with cerebral palsy.
Generally, the prescribed dosage of oxiracetam is 800–2400 mg per day, with gradual dose escalation after initiation. In a randomized, double-blind, placebo-controlled trial evaluating the clinical efficacy and safety of oxiracetam for cerebral palsy, 30 patients were enrolled to receive the drug. After four weeks of treatment, patients showed significant improvements in both intelligence scores on the Wechsler Preschool and Primary Scale of Intelligence (WPPSI) and activities of daily living (ADL) scores.
Cerebrolysin, nerve growth factor, gangliosides, and lysine may also have potential therapeutic effects on early childhood cerebral palsy. Cerebrolysin is a neuropeptide with neurotrophic and neuroprotective properties. It inhibits apoptosis, enhances synaptic plasticity, and induces neurogenesis; it also promotes the proliferation, differentiation, and migration of neural progenitor cells, leading to favorable neurological outcomes.
In a controlled study involving 120 infants with severe perinatal brain injury, the patients received intracerebral injections of Cerebrolysin at a dose of 0.1 mL/kg body weight, twice weekly for five weeks. The efficacy of the intervention was assessed using baseline scores from the Communication and Symbolic Behavior Scales (CSBS).Three months later, the social skills, speech, symbolic behavior, and total scores in the Cerebrolysin group increased by 65.44%, 45.54%, 358.06%, and 96.00%, respectively, compared with baseline scores.Additionally, a study reported that acupoint injection of Cerebrolysin in a child with cerebral palsy over an 8-year period resulted in significant improvements in both functional and cognitive outcomes.
The basic mechanism of action of gangliosides is similar to that of Cerebrolysin. However, gangliosides also play a significant role in neurotransmission. In an experimental study, neonatal rats with hypoxic-ischemic injury were administered ganglioside GM1. After 26 days of treatment, the experimental group demonstrated improved neurobehavioral function compared to the control group, as evidenced by performance in the hanging test, inclined plane test, and open field test.
Darbepoetin and erythropoietin are also used as neuroprotective agents. They possess anti-inflammatory and anti-apoptotic properties, which can improve cognitive function in infants. In a study involving preterm infants, none of the infants treated with erythropoietin developed cerebral palsy, whereas five cases occurred in the placebo group.
Cell Therapy
Over the past decade, cell therapy has rapidly evolved into a potential treatment for various neurological disorders, including cerebral palsy. Medical professionals are conducting experiments with different types of cells to investigate their therapeutic benefits in the treatment of cerebral palsy.Numerous animal studies have demonstrated the efficacy of cell therapy in cerebral palsy, but few human studies have been published in this area to date.Here, we list several cell types used for the treatment of cerebral palsy, as detailed below.
I. Bone Marrow Monocytes
Bone marrow is a mixture of various cell types that can be used for regeneration. Bone marrow stem cells can differentiate into multiple cell types, including blood cells and neural cells. Mononuclear cells can be isolated using density gradient centrifugation; these cells contain various progenitor cells, such as hematopoietic stem cells, mesenchymal stem cells (MSCs), endothelial progenitor cells, and very small embryonic-like stem cells.
Researchers conducted a clinical study on 71 pediatric patients with incurable neurological disorders, including 20 children with cerebral palsy. The intervention involved intrathecal injection of autologous bone marrow mononuclear cells. Regular follow-ups (mean follow-up duration: 15 ± 1 months) revealed symptom improvement in 80% of the patients, with no major adverse events observed. A subsequent study by the same team two years later analyzed an additional 108 pediatric patients, among whom 92.6% exhibited symptom improvement.
The team also presented two pediatric cases of cerebral palsy treated with autologous bone marrow mononuclear cells. Follow-up records at 6 months showed significant changes and improvements in the children’s intelligence quotient (IQ) and Functional Independence Measure (FIM) scores. In a case report submitted by another research team, a child with cerebral palsy who received autologous bone marrow mononuclear cell therapy demonstrated improvements in motor, sensory, cognitive, speech, and bowel and bladder functions.
II. Bone Marrow Stromal Cells
Eighteen children with cerebral palsy received treatment with autologous bone marrow-derived total nucleated cells administered via percutaneous and intravenous routes. The results showed an overall increase of 4.7 months in developmental age, as assessed by the Battelle Developmental Inventory. Furthermore, the study indicated that this procedure is relatively safe for use in children with cerebral palsy.
Researchers conducted a study in which children with moderate to severe cerebral palsy were administered neural stem cell-like cells derived from their own bone marrow mesenchymal tissue. At the 6-month follow-up, these patients showed a significant improvement in Gross Motor Function Measure (GMFM) scores, with no serious adverse events reported. A similar result was obtained in a study conducted by another research team.
III. Human Umbilical Cord Blood Cells
Hematopoietic, endothelial, epithelial, and neural tissues can all be derived from umbilical cord blood cells, although the quantity of stem cells isolated from umbilical cord tissue is 10% lower than that from bone marrow. Researchers have reported the efficacy of allogeneic umbilical cord blood cells against John Cunningham (JC) virus and herpesvirus infections. In one study, two children with spastic diplegic cerebral palsy were treated with autologous umbilical cord blood cells; follow-up assessments indicated improvements in various motor function metrics, with no significant adverse events observed. For further details on umbilical cord blood cell research, please refer to VCBeat’s previous article: “Controversial Research on Umbilical Cord Blood Hematopoietic Stem Cells May Bring New Hope for Cerebral Palsy Treatment.》
Another study reported that a two-and-a-half-year-old boy treated with intravenous autologous umbilical cord blood mononuclear cells showed improved motor control, reduced spastic paralysis, and regained vision within two months. At 40 months of age, the child was able to walk with a gait trainer, crawl, feed himself independently, and move from a prone position to sitting. His receptive and expressive language skills also improved, enabling him to understand four-word sentences and a vocabulary of 200 words. Additionally, his electroencephalogram (EEG) findings showed improvement.
Another research team attempted to treat a 5-year-old girl with multiple intravenous and intrathecal injections of umbilical cord mesenchymal stem cells derived from her younger sister. Following the treatment, the patient’s cerebral palsy symptoms improved. Subsequent observation over 28 months demonstrated that her immune function improved alongside enhancements in motor function, speech, physical strength, and cognitive abilities.
IV. Neural Progenitor Cells
In one study, 45 children diagnosed with cerebral palsy were all administered neural progenitor cells derived from aborted fetal tissue. One-year follow-up showed that, compared with the control group, these patients exhibited improvements in both motor and cognitive functions, demonstrating the safety and efficacy of this approach. In another study involving 30 children with cerebral palsy, researchers administered neural stem cell–like cells derived from autologous bone marrow mesenchymal stem cells. Compared with the control group, the treatment group showed improvements in language quotient and Gross Motor Function Measure (GMFM) scores, with no adverse events recorded. This indicates that neural stem cell–like cells are safe and effective in the treatment of cerebral palsy.
In another double-blind randomized controlled trial, allogeneic umbilical cord blood cells enhanced with recombinant human erythropoietin were transplanted into 40 children with cerebral palsy; following treatment, the patients’ cognitive and motor impairments improved, and positive changes in brain metabolism and structure were observed.
V. Olfactory Ensheathing Cells
From November 2001 to January 2008, a total of 1,255 patients with central nervous system disorders (including 68 children with cerebral palsy) underwent fetal olfactory ensheathing cell transplantation. Based on further observations, researchers concluded that transplanting olfactory ensheathing cells into the brain and spinal cord is safe and feasible, and can improve head and neck movement, phonation, and swallowing function to some extent, alleviate muscle spasticity and/or slow progressive deterioration, thereby enhancing the quality of life for children with cerebral palsy.
Among all the different types of cells used for cell therapy, autologous bone marrow mononuclear cells are the most frequently utilized; this is due to their ease of acquisition, abundant availability, and safety profile. Unlike embryonic cells, autologous bone marrow mononuclear cells are not tumorigenic and do not raise ethical or moral concerns.
To maximize the therapeutic efficacy of injected cells, selecting the optimal route of administration is crucial. Cells can be administered via intravenous, intrathecal, or intracerebral injection. The intravenous route is the least invasive; however, cells often become trapped in the pulmonary circulation, thereby compromising their therapeutic efficacy. Intrathecal administration is considered the optimal approach, as it is relatively minimally invasive and allows cells to effectively migrate to the injured tissue. Intracerebral injection is the most traumatic and increases the risk of secondary injury to surrounding tissues; therefore, this route of administration is not recommended.
Other Therapies
I. Hypothermia
Currently, researchers are exploring hypothermia as a treatment for hypoxic-ischemic encephalopathy (HIE), with promising results. This approach can reduce glutamate release, secondary energy failure, and free radical damage, while normalizing protein synthesis. Evidence suggests that hypothermia exerts neuroprotective effects by mitigating neurodevelopmental impairments, significantly lowering extracellular levels of excitatory neurotransmitters, and promoting neuronal survival. Combining hypothermia with other therapies, such as cell therapy, erythropoietin, and helium, may be more effective in addressing activated cell death pathways.
II. Hyperbaric Oxygen Therapy
A longitudinal controlled study in patients with cerebral palsy demonstrated that those receiving rehabilitation therapy combined with hyperbaric oxygen therapy (HBOT) showed greater improvement in Gross Motor Function Measure (GMFM) scores compared to the control group receiving rehabilitation therapy alone. However, early studies also indicated that HBOT monotherapy did not yield significant therapeutic benefits in patients with cerebral palsy. Therefore, the efficacy of HBOT in the treatment of cerebral palsy remains uncertain, warranting further research.
Although decades of research have yielded significant advances in clinical strategies for neurological recovery, the road ahead remains long and arduous. While research in this field has transitioned from the laboratory to the clinic, further accumulation of evidence is still required to draw definitive conclusions. As cell therapy and pharmacological interventions are currently the primary approaches for neurological recovery, key parameters such as optimal dosing, routes of administration, effective cell types, and timing of delivery require further investigation to maximize their efficacy. These studies should incorporate functional neuroimaging or biomarkers (e.g., cytokines, chemokines, and growth factors) to capture their impact on patients’ neurological recovery.
With the advancement and continued refinement of digital health technologies, an increasing number of digital therapeutic approaches have emerged alongside conventional treatments for cerebral palsy. Robotic assistants, mobility aids, and smart spoons are becoming increasingly indispensable components in the treatment of cerebral palsy in both children and adults, offering new hope for improving the daily lives of patients with this condition.
1. Robot Assistant Darwin

Robot Assistant Darwin
The adorable robot in the image is named “Darwin,” a physical therapy robotic assistant specifically designed and manufactured for children with cerebral palsy. Just as healthy children need homework to help them consolidate what they have learned, children with cerebral palsy sometimes require guidance and encouragement during physical therapy. Researchers at the Georgia Institute of Technology in the United States believe that robots like Darwin can play a positive role in encouraging children to engage in physical therapy.
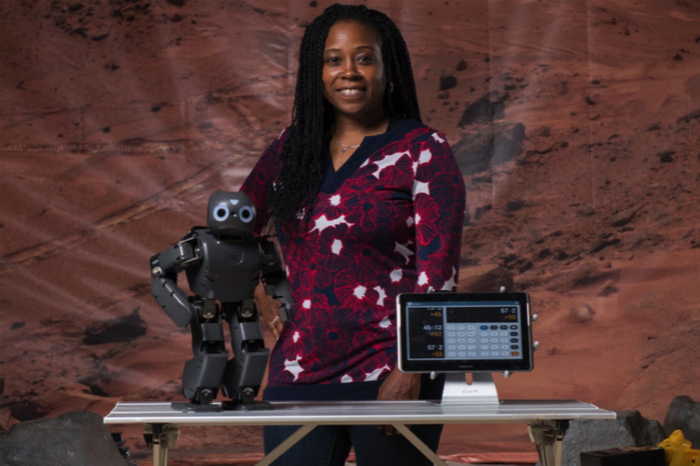
Ayanna Howard, Head of the Darwin Project, and Her Robots
Professor Ayanna Howard introduced that this type of socially interactive robot enables children with disabilities to receive therapy at home. The robotic assistant, Darwin, is designed for children with cerebral palsy, autism spectrum disorder, and those recovering from traumatic brain injury. It interacts with pediatric patients much like a clinician, monitoring their performance and providing motivational and corrective feedback.
In an experiment conducted by Howard and colleagues, a 3D motion tracker was used to monitor participants’ movements, while Darwin provided encouragement during task performance and demonstrated correct techniques when errors occurred. With the exception of one case, the robot demonstrated a significant positive impact on children’s physical activity.
According to Howard, they are currently piloting this technology in select clinics and within the homes of children with cerebral palsy. Current test results indicate that children with cerebral palsy can successfully adhere to the treatment plans and guidance provided by their robotic companions. The team’s next objective is to implement a two-month long-term pilot program to evaluate the full potential of the robot. Once the efficacy of robot-assisted therapy is validated, the technology will be ready for commercialization.
Although robots like Darwin are still unable to fully replace human physical therapists, they serve as valuable assistive tools that provide meaningful support to healthcare professionals, patients, and their families. After all, having a robotic companion is the dream of many children; how could Darwin, with its endearing charm and cool appeal, fail to win their affection?
2. Mobility Assistance Devices

Pediatric Patients Wearing Mobility Assistance Devices
Cerebral palsy can be caused by many factors, including brain injury at birth, infections, and trauma, and it is often difficult to diagnose before an infant reaches one year of age. Therefore, medical professionals believe that early intervention for cerebral palsy can better improve children’s various abilities. In recent years, a team of biomedical engineers and physical therapists from the University of Oklahoma has developed a motorized device to help infants at risk of cerebral palsy develop their motor and cognitive skills.
Thubi Kolobe, a core member of the team, is a physical therapist and researcher. As early as her tenure at the University of Illinois in Chicago, she developed a motor assessment to predict which preterm infants were most likely to develop cerebral palsy or other developmental disorders. After identifying these at-risk infants, Kolobe chose to intervene during a critical period of infant development (between 2 and 8 months of age), when children begin to learn kicking, moving, and crawling. Infant mobility is not only crucial for the development of motor skills but also plays a pivotal role in brain development.
As infants explore the world around them, they forge new neural connections and develop various cognitive skills, such as spatial awareness, problem-solving, and depth perception. Crawling is often a reward-based learning process. Consequently, if an infant attempts to move but fails to achieve the desired outcome, they may cease their efforts. Similarly, in many children with cerebral palsy who do not begin crawling until the average age of two, the brain ultimately prunes the neural connections associated with movement and spatial processing.
In 2003, Kolobe joined the University of Oklahoma. She soon began collaborating with a group of engineering professors at the university—Andrew Fagg, David Miller, and Lei Ding—to develop a device that helps infants at risk of developmental disorders explore their environment through crawling and receive positive feedback, thereby promoting brain development and accelerating the acquisition of motor skills.
The device has now reached its third iteration, featuring a cushion equipped with a three-wheel steering system, 12 built-in motion sensors, and a sophisticated machine learning algorithm. The built-in motion sensors transmit measurement data to a computer at a frequency of 50 times per second, generating a 3D movement visualization of the child on a nearby monitor. Additionally, cameras mounted on the device can capture the infant’s limb movements over a specified period.
More importantly, motion sensor data is processed by machine learning algorithms that can determine what the infant is attempting to do through computational analysis. The device then provides guidance in the appropriate direction, thereby rewarding the infant's attempts.
Therefore, if an infant attempts to kick with her hind legs but lacks sufficient strength for actual locomotion, the device will assist in moving her a few inches in the desired direction; if she waves an arm to move toward one side, the device can also rotate her in that direction almost simultaneously. Pilot tests indicate that infants wearing the device exhibit more limb movements than those who do not.
Funded by the National Robotics Initiative of the U.S. National Science Foundation, the team conducted a large-scale trial involving 56 infants aged 4 to 8 months. This time, the device also included a small cap adorned with dozens of small electroencephalogram (EEG) electrodes to detect their brain activity in real time as they moved. Researchers hope to create a “brain-computer interface” using the collected data; in the future, the device is expected to predict infants’ movement intentions solely based on their brainwaves.
Smart Spoon
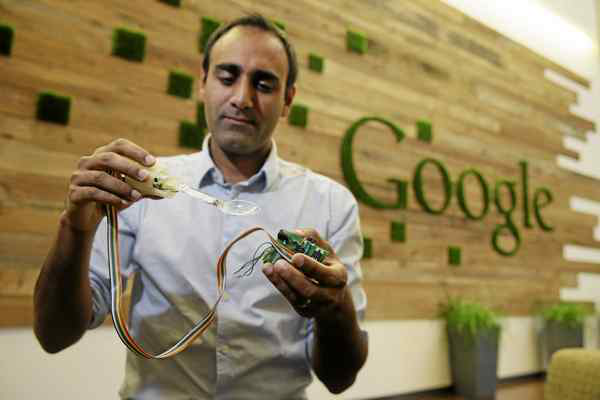
Anupam Pathak Demonstrates the Prototype of the Smart Spoon He Developed
In addition to restorative treatments and supportive care for children with cerebral palsy, many researchers have also turned their attention to improving the daily lives of adults with the condition. Anupam Pathak, a senior hardware engineer at Google, and his colleagues have developed a smart spoon that assists people with eating.
Tyrone Cobb is a 40-year-old patient with cerebral palsy. For decades, Cobb has been accustomed to eating only finger foods, such as pizza, hot dogs, and French fries; if he needs to dine out, he requires assistance from someone by his side. When he was fortunate enough to become one of the trial users of Liftware Level, a smart spoon newly developed by Verily (formerly Google’s life sciences division), the dining difficulties that had plagued him for forty years were finally resolved.
The smart spoon, named Liftware Level, offers an enhanced dining experience for individuals with limited mobility in their hands and arms. Its sleek design bears a resemblance to an electric toothbrush equipped with smartphone technology. Inside, the spoon houses sensors identical to those found in smartphones, which communicate with a microcomputer. By rapidly exchanging data with the computer, the device calculates hand and arm movements to keep the utensil consistently level. With this innovation, patients with cerebral palsy, such as Cobb, no longer need to worry about spilling their food.
Anupam Pathak, the technical lead of the project, stated that the smart spoon can perform thousands of motion calculations per second, making issues such as food spillage virtually impossible when using the device.
Verily officially launched Liftware Level in December 2016. Its website indicates that the smart spoon is expected to be priced at $195. Users can remove the spoon head and attach a fork in its place during use. Pathak stated that the company is exploring other applications for the device.