China's State Council Releases Key Healthcare Reform Tasks for 2017 with Clear Timelines and Roadmaps
VCBeat (WeChat ID: vcbeat) reports: On the afternoon of May 5, the State Council issued relevant documents outlining requirements for key healthcare reform tasks and priorities in 2017. The directives cover areas ranging from pharmaceuticals and medical services to healthcare payment systems, with some specifying the responsible departments and timelines for issuing detailed implementation guidelines.
A review of historical records by VCBeat reveals that since 2012, the State Council has annually issued a notice on key tasks for healthcare reform during this period, serving as the overall plan for advancing healthcare reform throughout the year. In recent years, terms such as medical consortia, private healthcare, separation of prescribing from dispensing, and health insurance cost containment have frequently appeared, reflecting the priority areas for healthcare reform.
So, what are the key tasks of this year’s “healthcare reform”? Will they represent the development direction of the healthcare industry in the coming period? The Key Tasks for Deepening Healthcare System Reform in 2017 is divided into two parts: one comprises the documents to be studied and issued this year, and the other covers the key initiatives to be promoted and implemented this year.
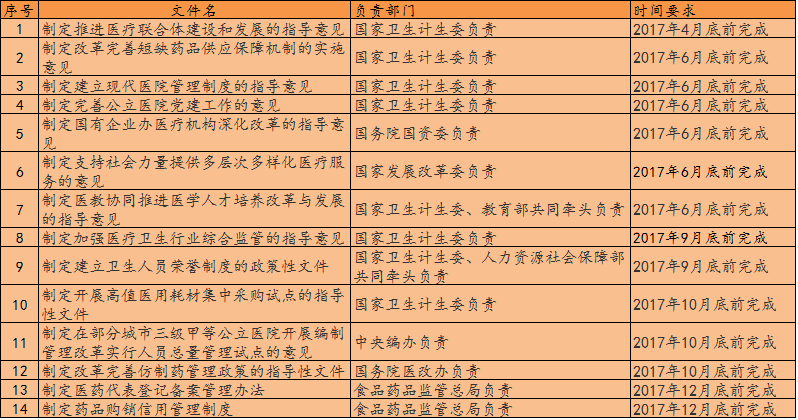
"Documents Required to Be Studied and Formulated by the State Council’s Healthcare Reform Office in 2017"
“Mission” requires adherence toUphold basic coverage, strengthen primary care, and establish robust mechanisms; deepen coordinated reforms in healthcare delivery, health insurance, and pharmaceuticals., advanceThe Establishment of Five Systems: Tiered Diagnosis and Treatment, Modern Hospital Management, Universal Health Insurance, Drug Supply Assurance, and Comprehensive Regulation。
In addition to the specific documents slated for release, the “Tasks” also clarify the key priorities to be advanced and implemented this year.
Key Tasks for Implementation
15. Summarize and promote successful local experiences, and further expand the scope of pilot programs.Pilot programs for tiered diagnosis and treatment and family doctor contract services expanded to over 85% of prefecture-level cities. (The responsibility lies with the National Health and Family Planning Commission.)
16. Implement the “Guiding Opinions on Promoting Family Doctor Contract Services” issued by the State Council’s Office of Healthcare Reform and other relevant departments; vigorously promote family doctor contract services, and improve policies related to payment and fee collection, performance evaluation, incentive mechanisms, and medical insurance. Prioritize key populations—including the elderly, pregnant and postpartum women, children, persons with disabilities, as well as patients with chronic diseases and severe mental disorders—and strengthen the delivery of family doctor contract services based on their needs.In 2017, the coverage rate of contracted services for key populations exceeded 60%., and include all impoverished populations within the scope of family doctor contract services. (The National Health and Family Planning Commission is responsible.)
17. Comprehensively launch pilot programs for the construction of medical consortia in various forms. All tertiary public hospitals must participate and play a leading role. Establish assessment and incentive mechanisms to facilitate the vertical integration of high-quality medical resources, enhance service capacity at the primary care level, and enable patients to access medical care conveniently in their vicinity. Explore the implementation of global budget payments under medical insurance and other payment models for division-of-labor and collaboration arrangements, such as vertically integrated medical consortia.Promote medical consortia to become communities of service, responsibility, shared interests, and management.Pilot integrated service models covering diagnosis and treatment, rehabilitation, and long-term care. By the end of June 2017, all provinces (autonomous regions and municipalities) shall formulate work plans to advance the development of medical consortia. In each province designated as a pilot for comprehensive healthcare reform, every prefecture-level city, as well as each pilot city for tiered diagnosis and treatment, shall establish at least one medical consortium with demonstrable effectiveness. (Led by the National Health and Family Planning Commission, in collaboration with the Ministry of Human Resources and Social Security, the State Administration of Traditional Chinese Medicine, and the Ministry of Finance; the department listed first shall serve as the lead agency, as applicable hereinafter.)
18.Organize and Launch Pilot Programs for Day Surgery in Tertiary Hospitals, further improve and implement policies on medical insurance payment and pricing of medical services. Implement various policies to guide and promote the participation of public hospitals in tiered diagnosis and treatment. (Responsible departments: National Health and Family Planning Commission, Ministry of Human Resources and Social Security, National Development and Reform Commission, State Administration of Traditional Chinese Medicine)
19. Strengthen the comprehensive capacity and discipline development of county-level public hospitals, and enhance the construction of clinical departments specializing in common and frequently occurring diseases within counties, as well as scarce specialty clinical disciplines. Promote full coverage of telemedicine in county hospitals located in impoverished counties. (The National Health and Family Planning Commission and the National Development and Reform Commission are responsible.)
20. Fully implement the “13th Five-Year” Action Plan for the Project to Enhance Traditional Chinese Medicine Service Capacity at the Primary Care Level. (Responsible agency: National Administration of Traditional Chinese Medicine)
21. Urge all provinces, cities, and counties to respectively improve and implement relevant plans for the healthcare service system, clearly defining the functional roles of medical and health institutions at all levels and types.Reasonably Control the Number and Scale of Public General Hospitals. (Responsible entities: National Health and Family Planning Commission, National Development and Reform Commission, and State Administration of Traditional Chinese Medicine)
22. Expand the scope of comprehensive reform demonstration for county-level public hospitals, with at least one national-level demonstration county in each province. Launch the comprehensive reform demonstration work for urban public hospitals. (National Health and Family Planning Commission and Ministry of Finance are responsible)
23. Clarify the policy measures for hospitals under the jurisdiction or administration of the National Health and Family Planning Commission and the State Administration of Traditional Chinese Medicine to participate in the comprehensive reform of local public hospitals, and carry out comprehensive performance assessments. Pilot provinces for comprehensive medical system reform shall select at least one prefecture-level city to conduct pilot performance assessments and intensify exploration efforts. (Responsible entities: National Health and Family Planning Commission, State Administration of Traditional Chinese Medicine, State Commission Office for Public Sector Reform, Ministry of Finance, National Development and Reform Commission, Ministry of Human Resources and Social Security)
24. AdvancementMilitary Hospitals and Armed Police Hospitals Participate in the Comprehensive Reform of Public Hospitals in Their Host Cities, and incorporate them into regional health planning and the tiered diagnosis and treatment system. (Responsible for by the Health Bureau of the Logistics Support Department of the Central Military Commission)
25. By the end of September 2017, comprehensively roll out the comprehensive reform of public hospitals across China.All public hospitals have completely eliminated drug markups.(excluding Chinese herbal decoction pieces). Coordinate and advance reforms in management systems, medical service pricing, personnel compensation, pharmaceutical distribution, and health insurance payment methods. Gradually increase the proportion of income from medical services in the total revenue of hospitals. By 2017, the ratio of pharmaceutical expenditures (excluding Chinese herbal decoction pieces) to total hospital costs in public hospitals across the first four batches of 200 pilot cities was reduced to approximately 30%, and the cost of sanitary materials consumed per RMB 100 of medical income (excluding income from pharmaceuticals) was reduced to below RMB 20. (Responsible entities: National Health and Family Planning Commission, State Administration of Traditional Chinese Medicine, National Development and Reform Commission, Ministry of Finance, Ministry of Human Resources and Social Security, Ministry of Commerce, State-owned Assets Supervision and Administration Commission of the State Council, and Health Bureau of the Logistics Support Department of the Central Military Commission)
26. Implement policies for reforming medical service pricing, comprehensively roll out pharmaceutical and medical service price reforms in urban public hospitals, and establish a regional coordination mechanism for medical service prices. (Responsible entities: National Development and Reform Commission, National Health and Family Planning Commission, Ministry of Human Resources and Social Security, State Administration of Traditional Chinese Medicine)
27. Fully implement the government’s investment policy for public hospitals that comply with regional health planning, and promote the establishment of a new compensation mechanism for public hospitals based on two channels: service fees and government subsidies.Gradually repay and resolve the long-term debts of eligible public hospitals.(Ministry of Finance, National Health and Family Planning Commission, State Administration of Traditional Chinese Medicine, National Development and Reform Commission)
28. Promote the establishment of a modern hospital management system. Pilot provinces for comprehensive medical reform shall select certain prefecture-level and above cities to conduct pilots, initially establishing a management and governance mechanism in which decision-making, execution, and supervision are coordinated, provide checks and balances, and mutually reinforce one another. Launch pilots on formulating articles of association for public hospitals. (The National Health and Family Planning Commission, the Ministry of Finance, the Ministry of Human Resources and Social Security, and the State Commission Office for Public Sector Reform are responsible.)
29.Launch Pilot Programs for Salary System Reform in Public Hospitals, promptly summarize the pilot experience and begin drafting guiding documents on personnel and compensation systems tailored to the characteristics of the healthcare industry. (Responsible entities: Ministry of Human Resources and Social Security, Ministry of Finance, National Health and Family Planning Commission, and State Administration of Traditional Chinese Medicine)
30. Each province (autonomous region, municipality) shall set annual targets for controlling the growth of medical expenses,In 2017, the average growth rate of medical expenses in public hospitals across China was kept below 10%.. Regularly publish the rankings of key monitoring indicators for each province (autonomous region, and municipality). (The National Health and Family Planning Commission, the Ministry of Finance, and the State Administration of Traditional Chinese Medicine are responsible.)
31. Complete the integration of the basic medical insurance systems for urban and rural residents, and implement the “six unifications” policy covering scope of coverage, financing policies, benefit packages, medical insurance catalogs, designated provider management, and fund management. Streamline the administrative system; pilot programs may be launched to establish Medical Insurance Fund Management Centers, which would assume responsibilities such as fund payment and management, drug procurement and expense settlement, negotiation of medical insurance payment standards, and agreement-based management and settlement with designated institutions. Improve the critical illness insurance system by adopting measures such as lowering deductibles, increasing reimbursement ratios, and reasonably defining the scope of eligible medical expenses, thereby enhancing the precision of payments under critical illness insurance for individuals in financial difficulty. (The Ministry of Human Resources and Social Security, the National Health and Family Planning Commission, and the China Insurance Regulatory Commission shall each take responsibility, with participation from the Ministry of Finance.)
32.The fiscal subsidy for urban and rural resident basic medical insurance has been increased from 420 yuan to 450 yuan per person per year., while simultaneously raising individual contribution standards and expanding the scope of medication coverage. (The Ministry of Finance, the Ministry of Human Resources and Social Security, and the National Health and Family Planning Commission shall be responsible respectively.)
33. Comprehensively advance the establishment of a diversified, composite health insurance payment system with diagnosis-related group (DRG) payment as the primary method.The Nation Selects Certain Regions to Pilot Diagnosis-Related Groups (DRGs) Payment, and encourage other regions to actively explore innovative approaches. Guide localities in improving various payment methods, including diagnosis-related group (DRG) payment, capitation, and per-diem payment. Pilot provinces for comprehensive medical system reform should select one or two prefecture-level cities to fully implement health insurance payment method reforms, covering all medical institutions and medical services within their jurisdictions, and significantly reducing the proportion of fee-for-service payments. (The Ministry of Human Resources and Social Security, the National Health and Family Planning Commission, and the Ministry of Finance shall be jointly responsible.)
34.Promote the Implementation of Diagnosis-Related Group (DRG) Payment, by the end of 2017, all cities shall implement diagnosis-related group (DRG) payment for no fewer than 100 disease categories. (Responsible entities: National Development and Reform Commission, National Health and Family Planning Commission, Ministry of Human Resources and Social Security, National Administration of Traditional Chinese Medicine, and Ministry of Finance)
35. Launch pilot programs for payment standards of drugs covered by medical insurance, and explore the formulation of payment standards for medical services under medical insurance.Promoting Nationwide Health Insurance Information Networking in China, to achieve direct settlement of inpatient medical expenses for cross-regional healthcare in accordance with referral regulations. (The Ministry of Human Resources and Social Security and the National Health and Family Planning Commission shall be responsible respectively.)
36. Develop approximately 200 clinical pathways, bringing the total to around 1,200, and formulate approximately 100 traditional Chinese medicine (TCM) clinical pathways. (The National Health and Family Planning Commission and the State Administration of Traditional Chinese Medicine shall be responsible respectively.)
37. Promote the implementation of the “Notice on Further Strengthening the Effective Coordination between Medical Assistance and Critical Illness Insurance for Urban and Rural Residents” issued by the Ministry of Civil Affairs and other departments, so as to enhance the synergistic effect of social protection. (Responsible entities: Ministry of Civil Affairs, Ministry of Human Resources and Social Security, National Health and Family Planning Commission, China Insurance Regulatory Commission, State Council Leading Group Office of Poverty Alleviation and Development, and Ministry of Finance)
38.Expand the Pilot Policy on Individual Income Tax Deductions for Commercial Health Insurance to Nationwide Implementation. (The Ministry of Finance, the State Administration of Taxation, and the China Insurance Regulatory Commission shall be responsible.)
39. Summarize experience and, in accordance with relevant regulations on government procurement of services, support the participation of commercial insurance institutions and other social forces in the administration of medical insurance. (Responsible entities: Ministry of Human Resources and Social Security, National Health and Family Planning Commission, China Insurance Regulatory Commission)
40. Deepen the implementation of health poverty alleviation programs, and strive to address the issues of rural impoverished populations falling into or returning to poverty due to illness. (Responsible entities: National Health and Family Planning Commission, State Council Leading Group Office of Poverty Alleviation and Development, National Development and Reform Commission, Ministry of Civil Affairs, Ministry of Finance, Ministry of Human Resources and Social Security, China Insurance Regulatory Commission, National Administration of Traditional Chinese Medicine, and Health Bureau of the Logistics Support Department of the Central Military Commission)
41. Promote the Precision Rehabilitation Services Action Plan to provide basic rehabilitation services for disabled persons in need. (Responsible entities: China Disabled Persons’ Federation, National Health and Family Planning Commission, Ministry of Finance)
42. Promote the implementation of long-term care insurance pilots. (Responsible entities: Ministry of Human Resources and Social Security, National Health and Family Planning Commission, Ministry of Civil Affairs, Ministry of Finance, and China Insurance Regulatory Commission)
43. Implement the “Several Opinions of the General Office of the State Council on Further Reforming and Improving Policies for Drug Production, Circulation, and Use” (Guo Ban Fa [2017] No. 13). Each province (autonomous region, and municipality directly under the Central Government) shall issue specific implementation plans for their respective regions by the end of June 2017, and promptly formulate detailed related policies and measures. (The National Health and Family Planning Commission, the China Food and Drug Administration, the Ministry of Industry and Information Technology, the Ministry of Commerce, the National Development and Reform Commission, and the Ministry of Human Resources and Social Security shall be respectively responsible.)
44.Accelerate the Consistency Evaluation of Quality and Efficacy for Generic Drugs. Launch pilot programs for the Marketing Authorization Holder (MAH) system for pharmaceuticals. (The China Food and Drug Administration is responsible.)
45. Further expand the scope of designated production for drugs in short supply, and support the establishment of centralized production bases for niche pharmaceutical products. Establish and improve a monitoring, early warning, and tiered response system for drugs in short supply. (The Ministry of Industry and Information Technology and the National Health and Family Planning Commission shall be responsible respectively.)
46. Make effective use of the National Comprehensive Management Information Platform for Drug Supply Guarantee, adhere to the principle of centralized volume-based procurement, promote the implementation of classified drug procurement in public hospitals, cultivate entities for centralized procurement, and encourage cross-regional joint procurement as well as joint procurement of drugs and high-value medical consumables by specialized hospitals. Research and develop a unified coding system for the procurement of high-value medical consumables; pilot provinces for comprehensive healthcare reform shall select several prefecture-level cities to conduct pilot programs for centralized procurement of high-value medical consumables, and other provinces are encouraged to launch similar pilots. (The National Health and Family Planning Commission is responsible.)
47. Implement the “Implementation Opinions (Trial) on Promoting the ‘Two-Invoice System’ in Drug Procurement by Public Medical Institutions” issued by the State Council’s Office for Healthcare Reform and other relevant entities. By the end of 2017, all public medical institutions in provinces designated as comprehensive healthcare reform pilots and in the first four batches comprising 200 pilot cities for comprehensive public hospital reform shall fully implement the “Two-Invoice System,” with other regions encouraged to adopt it. (Responsible entities: National Health and Family Planning Commission, China Food and Drug Administration, National Development and Reform Commission, Ministry of Industry and Information Technology, Ministry of Commerce, State Administration of Taxation, National Administration of Traditional Chinese Medicine, and Ministry of Finance)
48. Promote the establishment of a traceability mechanism for ex-factory drug pricing information. (The China Food and Drug Administration, the National Development and Reform Commission, the Ministry of Industry and Information Technology, the State Administration of Taxation, and the National Health and Family Planning Commission shall be responsible.)
49. Increase the number of drug varieties included in national price negotiations and ensure effective coordination between price negotiations and medical insurance policies. (The National Health and Family Planning Commission and the Ministry of Human Resources and Social Security are responsible.)
50. Pilot ImplementationClassified and Graded Management of Retail Pharmacies, Encouraging the Development of Chain Pharmacies, to explore the interconnectivity and real-time sharing of prescription information from medical institutions, medical insurance settlement information, and drug retail consumption information. (The Ministry of Commerce, the Ministry of Human Resources and Social Security, the National Health and Family Planning Commission, and the China Food and Drug Administration shall be responsible.)
51.Conduct assessments of the National Essential Medicines List and formulate incentive policies to prioritize the use of national essential medicines.. (Responsible by the National Health and Family Planning Commission)
52. Select certain regions to pilot the establishment of a hospital chief pharmacist system. (The National Health and Family Planning Commission is responsible.)
53. Promote the application of intelligent monitoring systems for medical insurance, covering most pooling regions by the end of 2017, and extend medical insurance oversight of healthcare institutions to include medical personnel. (The Ministry of Human Resources and Social Security and the National Health and Family Planning Commission shall be responsible respectively.)
54. Strengthen supervision and management of non-profit private medical institutions in terms of property rights ownership, financial operations, and the use of fund surpluses, and enhance control over the profit margins of for-profit medical institutions. (The National Health and Family Planning Commission and the Ministry of Finance are responsible.)
55.Launch pilot programs for privately operated TCM institutions and improve the record-filing management measures for TCM clinics. (The National Administration of Traditional Chinese Medicine is responsible.)
56. Urge localities to refine measures and, in accordance with the requirement to “allow medical and health institutions to exceed the current wage control levels for public institutions, and to use income from medical services—after deducting costs and setting aside various funds as prescribed—primarily for personnel rewards,” develop separate methods for determining the total amount of performance-based wages for medical and health institutions, and gradually increase the proportion of revenue from medical services, such as consultation fees, nursing fees, and surgical fees, in the total hospital revenue. Protect and mobilize the enthusiasm of medical personnel. (The Ministry of Human Resources and Social Security, the Ministry of Finance, and the National Health and Family Planning Commission shall each be responsible.)
57.Train more than 25,000 general practitionersContinue to implement the program for tuition-free training of rural-oriented medical students, enrolling and training approximately 5,000 undergraduate tuition-free medical students for central and western regions. Continue to organize and implement the special post program for general practitioners. Enroll an additional 70,000 physicians in standardized residency training. Advance pilot programs for the standardized training system for specialist physicians. Accelerate the cultivation of talent related to the development of the health industry. (The National Health and Family Planning Commission, the Ministry of Human Resources and Social Security, the Ministry of Finance, the Ministry of Education, and the State Administration of Traditional Chinese Medicine are responsible.)
58.The fiscal subsidy standard for per capita basic public health service funding has been raised to 50 yuan.Strengthen the disease prevention system and the chronic disease prevention and control system. Promote health effectively. (The Ministry of Finance, the National Development and Reform Commission, and the National Health and Family Planning Commission are respectively responsible.)
59. Optimize the proportion of senior and intermediate-level positions in primary healthcare institutions. Further reform and improve the professional title evaluation system for primary healthcare personnel. (Responsible units: Ministry of Human Resources and Social Security, National Health and Family Planning Commission)
60. Implement systems such as prescription reviews. Guide local authorities to compile specific lists of high-cost drugs, including adjuvant and nutritional agents, for key monitoring. (Responsibility: National Health and Family Planning Commission, State Administration of Traditional Chinese Medicine)
61. Gradually improve the provincial, municipal, and county population health information platforms, achieving interconnectivity between the national and provincial population health information platforms by 2017. Implement the national pilot work for the construction of health and medical big data centers and industrial parks. Accelerate the unification of relevant norms and standards, including medical record documentation guidelines, disease classification coding, surgical procedure coding, and medical nomenclature and terminology. (Responsible entities: National Health and Family Planning Commission, Ministry of Industry and Information Technology, National Development and Reform Commission, Ministry of Finance, National Administration of Traditional Chinese Medicine)
62. Relying on the National Clinical Medical Research Centers, enhance the diagnostic and treatment technical levels and service capabilities of primary healthcare institutions, and promote the establishment of a “precise matching” mechanism for health and medical technology assistance. Conduct major thematic research projects that support the deepening of healthcare reform. (Responsible entities: Ministry of Science and Technology, National Health and Family Planning Commission, Health Bureau of the Logistics Support Department of the Central Military Commission)
63. GuidancePilot Program for Electronic Licenses of Medical Institutions, Physicians, and Nurses in the Beijing-Tianjin-Hebei Region, pilot programs were rolled out in all provinces across China in 2017. (The National Health and Family Planning Commission is responsible.)
64. Continue to promote national-level pilot programs for the integration of medical and elderly care services, and advance such integration at the community and home-based levels. Launch initiatives for traditional Chinese medicine (TCM)-based healthy aging. Promote the integrated development of the health sector with related industries, and advance the establishment of demonstration bases for health and medical tourism. (Responsible entities: National Health and Family Planning Commission, Ministry of Civil Affairs, National Development and Reform Commission, State Administration of Traditional Chinese Medicine, and Ministry of Finance)
65. Continue to implement the Action Plan for Improving Medical Services.Building Harmonious Doctor-Patient Relationships. (The National Health and Family Planning Commission and the State Administration of Traditional Chinese Medicine are responsible.)
66. Promote the appointment of the principal leaders of local Party committees and governments, or one of their principal leaders, as the head of the healthcare reform leading group in each locality, to fully leverage the coordinating and facilitative role of these groups. (The State Council Healthcare Reform Office is responsible.)
67. Establish binding mechanisms, such as incorporating healthcare reform into the performance evaluation criteria for local governments. Clarify the responsibilities of local governments at all levels and relevant departments, ensuring that responsibilities are firmly assigned, requirements are practically defined, and assessments are rigorously implemented. Create a ledger of healthcare reform tasks, strengthen monitoring of reforms, and issue regular reports. (Responsibility: Local people’s governments at all levels)
68. Actively summarize and promote the successful experiences of healthcare reform from various regions. Provinces participating in comprehensive healthcare reform pilots shall play a demonstrative and leading role, accumulating experience for the overall reform. The number of provinces involved in comprehensive healthcare reform pilots shall be increased as appropriate. (The State Council Office for Healthcare Reform is responsible.)
69. Strengthen publicity and guidance for healthcare reform. Adhere to the correct orientation of public opinion, enhance positive publicity for healthcare reform, and provide thorough interpretations of key policy documents. Intensify training efforts on healthcare reform by conducting comprehensive training for personnel in relevant government departments, healthcare reform offices, and public hospital management teams. (Responsible entities: State Council Healthcare Reform Office, Publicity Department of the CPC Central Committee, Cyberspace Administration of China)
70. Strengthen supervision and evaluation of healthcare reform. With regard to the "Several Opinions on Further Promoting the Experience of Deepening Healthcare System Reform" forwarded by the General Office of the CPC Central Committee and the General Office of the State Council, as well as documents issued by entities such as the State Council’s Healthcare Reform Office on implementing “Two-Invoice SystemConduct special inspections on the implementation of the “Implementation Opinions (Trial).” Evaluate the reform progress in provinces piloting comprehensive medical system reforms, and organize mid-term evaluations of tiered diagnosis and treatment as well as performance assessments of the comprehensive reforms of urban and county-level public hospitals. (Responsibility: State Council Office for Medical System Reform)