Precise MD Submits IPO Prospectus: Pioneering AI-Driven Imaging Platform Aims to Eliminate Unnecessary Prostate Biopsies
Currently, there is no reliable clinical method for diagnosing malignant prostate cancer. In many cases, the proliferation and spread of cancer cells in the body are actually very slow and do not affect human health or life safety.
For malignant prostate cancer, the currently widely used prostate-specific antigen (PSA) test lacks diagnostic precision, and microscopic examination of cancer cells also fails to yield satisfactory results.。
How Is Prostate Cancer Best Diagnosed?
PSA testing measures the level of prostate-specific antigen; elevated levels indicate that the individual may be at risk for prostate cancer. Let us now use figures to intuitively demonstrate the accuracy of PSA testing. If 1,000 men undergo PSA testing, approximately 240 will be identified as having PSA levels suggestive of cancer risk.
Subsequently, biopsies are performed on these 240 individuals: a needle is inserted through the rectum to obtain tissue samples from multiple sites in the prostate for testing. Based on the biopsy results, 140 of these individuals are informed that they do not have cancer, with the explanation that the PSA test is not entirely accurate. The remaining 100 individuals have biopsy results confirming the presence of cancer cells; however, in as many as 50 of these cases, the cancer cells grow so slowly that they will never metastasize. This phenomenon is known as “overdiagnosis.”
Unfortunately, there is currently no effective way to distinguish whether these cancer cells are “indolent” or malignant. As a result, 80 out of the 100 patients would opt for surgery or radiation therapy, along with “active surveillance” (high-frequency PSA testing and biopsies).
As a result, 60 of them will develop urinary incontinence and sexual dysfunction as side effects of treatment. Among these 80 patients, only three achieve positive therapeutic outcomes; for the remaining 77, either their cancer would not have caused harm in the first place, or the disease had progressed too severely for treatment to be of any benefit.
Screening and treatment methods with such low accuracy may cause more harm to patients than cancer itself.
Demand Sparks a Hundred Schools of Thought
Researchers are currently developing various genetic testing methods, imaging technologies, and advanced algorithms akin to facial recognition. One such testing system, named Precise MD, analyzes green fluorescent images of prostate cells. Should these methods be implemented in clinical practice, which will reduce the number of prostate biopsies in the United States by at least 1 million cases annually and, more importantly, spare thousands of patients from undergoing unnecessary cancer treatments.
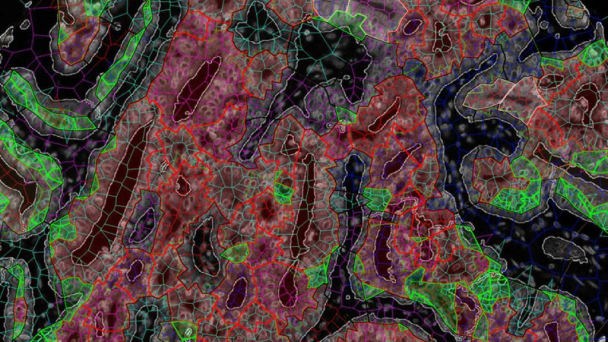
Precise MD Differentiates Benign and Malignant Prostate Cancer Cells Using Fluorescent Biomarkers and Other Characteristic Indicators
Fluorescent images of prostate cells resemble the shimmering jade necklaces worn by ancient emperors. If Dr. Gerardo Fernandez’s theory is correct, these images are even more valuable than gold and jade. These glowing images can identify which prostate cells pose no threat to human health, thereby sparing thousands of patients from unnecessary and burdensome treatments.
Dr. Laurence Klotz of Sunnybrook Health Sciences Centre in Toronto stated, “This field is currently very active; indeed, numerous blood and urine tests are already available for clinical use. Avoiding biopsies in patients with only slightly elevated PSA levels can largely prevent overdiagnosis.” Dr. Klotz’s own research has also demonstrated that most patients diagnosed with prostate cancer can rely on active surveillance to ensure the cancer does not spread, without the need for treatment.
PSA Testing: Angel or Devil?
The debate over PSA testing is currently intense. Opponents advise against undergoing the test, while proponents argue that such a stance would prevent many prostate cancer patients from learning their diagnosis in time, thereby delaying treatment.
PSA testing was introduced into clinical practice in the 1980s. Critics argue that this approach has led to overdiagnosis in millions of men, many of whom harbor prostate cancers that would never require treatment. Yet, a significant number of these men have spent the rest of their lives dealing with incontinence requiring adult diapers and even sexual dysfunction, with the culprit being not the cancer itself but the unnecessary treatments they received.
However, both sides of the debate acknowledge the following two facts. First, many patients with elevated PSA levels are found not to have cancer after biopsy, and this procedure, which involves inserting a needle into the rectum to extract tissue, may lead to infection and other adverse outcomes. Second, a significant proportion of patients do not require treatment even if diagnosed.
“This is a problem that has long plagued us; our cancer screening methods are indeed far from adequate,” noted Clare Tempany, a prostate cancer specialist at Brigham and Women’s Hospital in Boston. “Since PSA became notorious, there has been growing awareness that we need to employ more sophisticated approaches.”
Imaging Technology Could Be the Savior
In fact, many methods superior to conventional PSA testing have already emerged, and many people are no longer choosing to undergo biopsies. Doctors generally believe that a PSA level above 4 indicates a risk of cancer, but in reality, one-quarter of individuals with PSA levels between 4 and 10 do not have cancer.
For example, a blood test called the "Prostate Health Index" detects several forms of PSA, rather than just one as in traditional tests. This test can avoid approximately 36% of unnecessary biopsies but may also miss 2.5% of patients with malignant prostate cancer.
“There is also a blood test called the 4Kscore, which can detect malignant cancer cells more accurately than PSA, thereby avoiding up to 60% of unnecessary biopsies, but it may miss 5% of patients with malignant cancer,” commented David Penson, a urologist at the Vanderbilt-Ingram Cancer Center.
This situation has spurred researchers worldwide to strive for solutions, with many laboratories working to develop advanced imaging techniques to avoid unnecessary biopsies. One such approach is “multiparametric MRI” (MRI—Magnetic Resonance Imaging), which can assess the size and density of prostate cancer cells as well as their vascular supply.
Researchers from the Netherlands reported at the European Association of Urology Congress in March that multiparametric MRI can not only reduce unnecessary biopsies by 70%, but also achieve screening efficacy comparable to biopsy, without missing patients with malignant cancer.
At the annual meeting of the American Urological Association, studies on dozens of advanced MRI technologies will be discussed. Although many have corroborated the findings reported by Dutch researchers, there has also been considerable less-than-favorable feedback. For instance, one study found that advanced MRI techniques missed lesions in 63% of cases. In other studies, while MRI errors and omissions were less frequent, they still placed physicians in a dilemma, leaving them uncertain about whether to trust this diagnostic modality.
Dr. Anthony D’Amico of Brigham and Women’s Hospital in Boston gently pointed out, “The first step after detecting an elevated PSA is not to perform a biopsy but to undergo an MRI, which is currently still in the research phase.”
Therefore, physicians are eagerly awaiting the results of the large-scale clinical trial on MRI conducted by PRECISE. PRECISE is an experimental program designed to test the effectiveness of MRI, which was launched last year and led by Klotz. Based on earlier data, Klotz estimated, “MRI could help 250,000 men in the United States and Canada avoid unnecessary biopsies and hospitalizations each year, without compromising the accuracy of our clinical diagnosis of malignant cancers.”
However, behind the perfect clinical presentation lies a high cost: multiparametric MRI costs approximately $1,000 to $2,000 per scan. This has also driven researchers to explore other imaging modalities, in the hope of finding diagnostic methods that are both accurate and affordable. Dr. D’Amico stated, “There is now evidence suggesting that PET (positron emission tomography) and other imaging techniques can perform better.”
Prostate-specific membrane antigen (PSMA) is widely expressed on prostate cancer cells, whereas this protein is rare in healthy cells. PET scans can map the distribution of this protein, and the technology shows promise for predicting whether cancer has metastasized. Cancer cells confined to the gland are generally not dangerous, let alone fatal. Researchers are now focusing on identifying optimal radiotracers to enable more effective PET imaging of PSMA.
Jeffrey Karnes, a prostate specialist at the Mayo Clinic, stated, “The primary issue now is determining just how accurate PET scans can be. The hope for resolving this lies in the fact that malignant cancer cells absorb tracers more readily than indolent cancer cells.”
Genetic Testing Can Also Play a Role
Currently, there are no effective genetic testing methods available on the market to help men with elevated PSA levels avoid biopsy. However, Dr. Brian Helfand and his research team at North Shore University are developing a genetic technology that may fill this gap. Based on more than 100 DNA variants, this technology can identify the one-third of patients most likely to have aggressive prostate cancer, meaning that the remaining individuals could be spared from undergoing biopsy.
A 64-year-old patient had a PSA level of 4.6 ng/mL. Although this value was only slightly above the normal range, many physicians still recommended a biopsy. However, genetic testing revealed that his hereditary risk index was only 40%, which is below the threshold. “Other doctors he consulted all recommended a biopsy, but I advised him that it was unnecessary,” said Helfand.
At the American Urological Association Annual Meeting, European researchers will present a biomarker panel composed of six blood proteins. In their study of 474 men with prostate-specific antigen (PSA) levels between 2 and 10 ng/mL, 141 cases avoided biopsy, demonstrating significantly greater reliability than relying on PSA levels alone. They anticipate that this biomarker approach will effectively reduce the number of unnecessary prostate biopsies.
Another pressing issue in the PSA debate is that many men diagnosed with prostate cancer following a biopsy undergo unnecessary treatment, as their cancers are indolent. The currently used biopsy analysis system cannot reliably distinguish harmless cells from threatening cancerous ones.
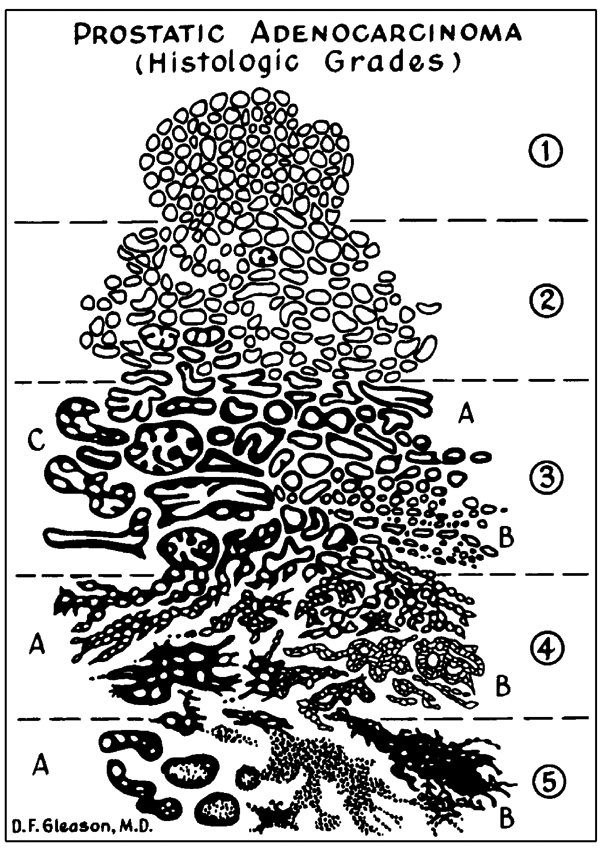 Gleason Scoring System: Grading and Classifying Prostate Cells Based on Morphology
Gleason Scoring System: Grading and Classifying Prostate Cells Based on Morphology
The Gleason scoring system, developed in the 1960s, relies on microscopic grading of stained prostate cells, with scores ranging from 2 to 10. Cells exhibiting regular morphology and less compact architecture are less likely to be malignant, typically receiving a score below 3.
Cells with irregular shapes, angular edges, or elongated forms that are tightly encapsulated are likely to be classified as malignant cancer cells. Klotz stated, “Grade 3 cells generally lack the ability to metastasize and do not pose a threat to health; however, Grade 4 cells are highly dangerous.”
However, in some male cases, the majority of cells are graded 3, but there are also some cells graded 4, which is referred to as Gleason score 3+4. In such situations, accurate diagnosis can be challenging. These cases typically undergo surgery or radiation therapy, or a combination of both, but most of the cells eliminated would not have posed a threat to their health.
Fortunately, genetic testing holds promise for distinguishing between benign cells and malignant cancer cells. Currently, at least three genetic tests are available for clinical use; these tests utilize liquid biopsy samples containing viable cells and perform analyses based on genes associated with malignant cancer cells.
Dr. Stacy Loeb, a urology specialist at NYU Langone Medical Center, pointed out: “Genetic testing can help us determine whether the cancer cells in patients in the ‘gray zone’ (Gleason score 3+4) are aggressive. The management of these Gleason 3+4 patients has long been a subject of controversy, and genetic testing may provide a decisive solution.” She will also present her research findings at the annual meeting of the American Urological Association, including a test called “Decipher,” which is set to change conventional thinking and enable patients inclined toward treatment to remain safe with active surveillance.
However, we must also acknowledge that genetic testing is expensive, costing between $3,000 and $4,000 per test, and it is not necessarily covered by health insurance. A more serious issue is that genetic testing cannot provide a definitive answer as to whether cancer cells are harmless. Instead, genetic testing can only indicate whether the individual has a very low, low, moderate, or high risk of developing highly metastatic cancer.
“The issue now is that genetic testing does not necessarily mitigate risk to a significant extent,” noted Karnes of the Mayo Clinic. “For instance, if a patient has a 30% pre-test risk of developing cancer, genetic testing might indicate a revised risk index of 35%. However, what we actually need are definitive answers—either 0% or 100%.”
Although genetic testing is not perfect, it can provide men with a reference to help them decide between undergoing treatment or opting for active surveillance. Duane Foulkes, 70, recently sold his factory in Madison, Wisconsin. At the time, his PSA level was 5, but it rose to 9 three months later, prompting him to undergo a biopsy at the Mayo Clinic. “His Gleason score was 6, and he immediately considered consulting me,” said Foulkes.
Genetic testing revealed that he had only a slow-growing, non-aggressive cancer, which gave him sufficient confidence to opt for conservative treatment and active surveillance.
Precise MD: Cutting-Edge Technology in Imaging and Algorithms
The prostate cell fluorescence images developed by Fernandez, as mentioned earlier, may yield superior results. These images, resembling jade necklaces, are actually generated by fluorescently labeling signaling molecules in prostate cells and then visualizing them under a microscope.

Dr. Gerardo Fernandez
Dr. Gerardo Fernandez earned his M.D. from Drexel University in Philadelphia in 1992. In the early stages of his career, he specialized in tumor pathology with a focus on cancer biomarkers at Impath’s commercial reference laboratory. Later, at Aureon Biosciences, he led a team of pathologists and imaging engineers dedicated to developing diagnostic and prognostic technologies based on multispectral fluorescence.
After leaving the East Coast, he served as Medical Director of the Pathology Department at Ventana for two years, continuing to develop medical image analysis technologies. He ultimately returned to Mount Sinai Hospital in New York, where he led the development of Precise MD technology.
In the Precise MD assay system, Fernandez and his colleagues at Mount Sinai Hospital in New York have identified five signaling molecules, including proteins produced by malignant cells, which can help distinguish between benign and malignant cells.
“Initially, we started with more than 10,000 feature indicators and then used AI computations to narrow the scope down to the 30 most optimal indicators. Based on these 30 indicators, we added dozens more according to imaging results, along with 5–10 additional variables such as individual PSA levels and age,” said Fernandez. “We then used AI to evaluate thousands of combinations, grouping together the most predictive indicators, and employed the resulting algorithm to calculate the likelihood of malignant cancer.”
Although Precise MD is still in the testing phase, early results indicate that this method offers a significant improvement over the Gleason scoring system in predicting malignant cancer.
“If large-scale trials in the later stages also demonstrate its efficacy, then I can confidently tell male patients that they can certainly opt for active surveillance,” Fernandez said optimistically. “This will truly transform the diagnosis and treatment pathway for prostate cancer.”
Source: STAT News; compiled by VCBeat.