Purui Genomics: Advancing Precision Patient Selection and Clinical Trial Success in Immuno-Oncology
Immunotherapy controls and kills tumor cells by activating the patient’s own immune system and enhancing anti-tumor immunity within the tumor microenvironment. However, immunotherapy has significant limitations: the response rate is not high, with only approximately 20%–40% of patients deriving therapeutic benefit. How, then, can treatment efficacy be predicted prior to therapy?
In 1891, New York orthopedic surgeon William Coley discovered that patients who developed postoperative infections after tumor resection surgery recovered better than those who did not. He then conducted a bold experiment—directly injecting streptococcus into tumor patients in the hope of treating their tumors.
Initially, Coley administered live Streptococcus bacteria to patients. However, after two patients died from bacterial infections following treatment, he switched to injecting a filtered mixture of heat-killed Streptococcus pyogenes and Serratia marcescens. Using this method, he treated 1,000 cancer patients, the majority of whom survived.
William Coley
This mixed bacterial vaccine is known as “Coley’s toxins,” and this potent bacterial injection therapy is hailed as the origin of tumor immunotherapy.
Immunotherapy—The New Mainstream in Cancer Treatment
More than a century later, following the advent of radiotherapy, chemotherapy, and targeted therapy, immunotherapy has emerged as a standout advancement in the field of oncology. In 2013, cancer immunotherapy was named one of the “Breakthroughs of the Year” by Science, marking its formal recognition as a legitimate therapeutic approach.
Deficiencies of Conventional Therapies and Targeted Therapy
Conventional therapies such as surgery, radiotherapy, and chemotherapy impose a significant burden on the body, and once malignant metastasis occurs, cure remains elusive regardless of the treatment modality. Targeted therapy emerged in the late 20th century. This approach enables the design of therapeutic agents that act at the cellular and molecular levels against well-defined oncogenic sites. In simple terms, targeted therapy is highly specific, selectively attacking cancer cells while sparing normal human cells. However, targeted therapy requires clearly defined targets, and the inevitable emergence of primary and acquired resistance to targeted drugs during treatment represents the greatest clinical limitation of this approach.
Limitations of Immunotherapy: Suboptimal Response Rates
Immunotherapy inherits the advantages of targeted therapy by enabling specific attacks on tumor cells. However, unlike targeted therapy, immunotherapy activates the patient’s own immune system to enhance anti-tumor immunity within the tumor microenvironment, thereby controlling and eliminating tumor cells. It is characterized by a longer response duration and significantly better resistance to drug resistance compared to targeted therapy, making it currently regarded as the most promising approach for cancer treatment.
However, immunotherapy has significant drawbacks: the response rate is low, with only approximately 20%–40% of patients deriving clinical benefit; while highly effective for some, it works only in a subset of individuals. How, then, can we predict treatment efficacy prior to initiating therapy?
Immunotherapy Requires Effective Predictive Tools for Early Assessment
Numerous studies and trials have demonstrated that patients with a higher number of somatic mutations, i.e., those with a high tumor mutational burden (TMB), exhibit better therapeutic responses. In other words, testing for mutations in patients' tumor tissues to assess TMB enables the early identification of individuals likely to benefit from treatment.
Purui Benchmark is an innovative precision diagnostics company based in Beijing. Leveraging cancer genomics, proteomics, and big data analytics, it provides precise analytical insights across various stages of oncology treatment for physicians and patients, facilitating the customization of personalized therapeutic regimens to maximize patient benefits.
In April 2017, the company launched China’s first precision diagnostic product specifically designed for cancer immunotherapy—“OncoBuster.” Leveraging multi-omics technologies, OncoBuster provides information such as predictions of therapeutic benefit for immune checkpoint monoclonal antibody therapy and immune cell therapy.
OncoStar is part of Purigen Bio’s multi-omics solution for precision diagnostics in tumor immunotherapy. By detecting tumor mutational burden (TMB) and tumor neoantigen burden (TNB) based on exome and transcriptome data, it accurately predicts whether patients will benefit from immune checkpoint inhibitors.
Compared with panel testing, whole-exome and transcriptome sequencing can more comprehensively identify neoantigens and accurately quantify tumor neoantigen burden, thereby providing a more realistic prediction of patient benefit.
Clinical Screening: Addressing the Limitations of Immunotherapy
Clinically, such testing protocols can significantly enhance the efficacy of immunotherapy. Although numerous genetic testing panels are currently available to guide cancer pharmacotherapy, they have predominantly focused on targeted therapy. As treatment paradigms shift, there is a growing array of not only targeted therapies but also personalized immunotherapy regimens. Consequently, in addition to existing assays for targeted drugs, there is an emerging clinical demand for screening tools tailored to immunotherapy.
On one hand, based on the provision of targeted therapy information, OncoStar Testing has pioneered a screening protocol for clinical immunotherapy. Although multiple PD-1 and PD-L1 inhibitors are currently available on the market, the cost of immunotherapy remains prohibitively high. If patients incur such substantial expenses without achieving therapeutic efficacy, while simultaneously missing the window for alternative treatment options, they would suffer significant harm.
Therefore, it is highly necessary to conduct such predictive testing prior to initiating immunotherapy. When Roche’s PD-L1 monoclonal antibody drug, atezolizumab, was launched, it was accompanied by a companion diagnostic for immunotherapy; specifically, pre-treatment testing for PD-L1 expression is mandatory, and the drug is indicated only when PD-L1 expression exceeds 50%.
Immunotherapy harnesses the body’s own immune system to attack tumor cells. Since each T cell possesses a unique T-cell receptor, sequencing and analysis of the T-cell immune repertoire can assess an individual’s immune potential. This approach not only enables early prediction of therapeutic efficacy in cancer patients but also allows for comprehensive monitoring of treatment response throughout the pre-, intra-, and post-treatment phases.
In addition to clinical screening, analytical research using patient samples can also provide data-driven support for clinical scientific research.
On the other hand, Oncostatin can also be used in immune cell therapy. Immune cell therapies, represented by CAR-T, have achieved exciting results in recent years. Many companies and hospitals are exploring this approach, giving rise to star companies such as Juno and Kite, with multinational corporations like Novartis also among the leaders. A report released this year by the Sinopharm Industry Research Center indicates that there are 305 CAR-T clinical trials worldwide.
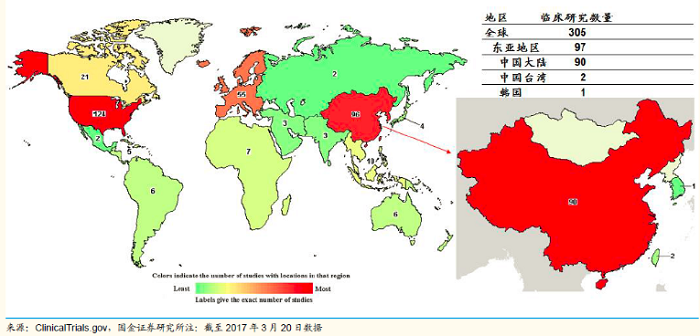
Source: ClinicalTrials, Sinolink Securities Pharmaceutical Industry Research Center
Next-generation cell therapy regimens require the identification of tumor neoantigens specifically expressed in patient tumor tissues. By using OncoStar, these tumor-specific antigens can be predicted, providing a reference basis.
Pharmaceutical R&D: Safeguarding Clinical Trials
Beyond clinical practice, diagnostic products can also provide robust support to pharmaceutical companies during the clinical trial phase. By conducting TMB/TNB testing on enrolled participants during clinical trials, it is possible to effectively predict treatment efficacy, identify patients likely to respond to therapy, and thereby enhance the likelihood of clinical trial success.
Take the pharmaceutical giant Bristol-Myers Squibb (BMS) as an example. In August 2016, BMS announced that its PD-L1 inhibitor Opdivo had failed in a Phase III clinical trial for non-small cell lung cancer (NSCLC). At that time, BMS used PD-L1 expression levels as the biomarker criterion, requiring all patients to undergo PD-L1 testing and administering the drug only to those with expression levels greater than 5%. However, the therapeutic efficacy in most patients was no better than that of chemotherapy. Subsequently, researchers raised the threshold to 50%, but the situation did not improve.
Many attribute the trial’s failure to Bristol-Myers Squibb’s flaws in experimental design—specifically, overly hasty patient selection. Currently, only about 20%–40% of patients truly respond to immunotherapy, which means that companies need to devote more time and effort to predicting therapeutic efficacy and also conduct diagnostic testing.
Timothy Byun, an oncologist at the University of California, St. Joseph Hospital, also stated, “The greatest limitation of this study is the uncertainty regarding which patients will respond to immunotherapy.”
At this year’s AACR annual meeting, Bristol-Myers Squibb presented a retrospective study that analyzed the Phase III CheckMate 026 clinical trial using tumor mutational burden (TMB) as a biomarker. When TMB was selected as the biomarker for treating non-small cell lung cancer (NSCLC), both the objective response rate (ORR) and overall survival (OS) associated with the therapy were significantly improved. This finding enhances the prospects for regulatory approval of the drug.
Currently, more than ten pharmaceutical companies in China are researching PD-1 and PD-L1 drugs, with over 20 clinical trials underway. The vast majority of these companies plan to use companion diagnostics to pre-stratify participants, thereby increasing the success rate of clinical trials.
Furthermore, although not all immunotherapy drugs are accompanied by companion diagnostics like Keytruda, due to the nature of immunotherapy, such companion diagnostics (whether PD-1 expression or PD-L1, or TMB/TNB testing based on exome and transcriptome as offered by companies like Purui Zhunke Technology) will gradually become a necessity in clinical practice, scientific research, and drug trials.
It is understood that Purui Benchmark has already established collaborations with multiple large hospitals in China. Moving forward, the company aims to expand its partnerships with hospitals and pharmaceutical companies to analyze patients who are currently using or will soon use immune checkpoint inhibitors. This initiative seeks to generate more data on immune checkpoint inhibitor therapy specific to the Chinese population, thereby enabling more targeted and precise evaluations of immunotherapy.