China's First 'White Paper on Primary Healthcare Innovation Industry' Officially Released
China’s healthcare services industry stands on the eve of profound transformation. With the frequent rollout of new healthcare reform policies—such as “promoting the establishment of a tiered diagnosis and treatment system,” “integrating medical care with elderly care,” “family doctor contract services,” and “advancing the development of medical consortia”—2017 is poised to become the inaugural year for the upgrading and leapfrog development of primary healthcare. Consequently, the entire healthcare industry will inevitably focus its attention on the primary care sector.
Since December 2016, VCBeat has focused closely on the primary healthcare sector. In February 2017, it took the lead in releasing the industry scan “Investment Opportunities in Primary Healthcare in 2017” and launched a nationwide call for submissions of “Best Practice Cases in China’s Primary Healthcare.” On May 17, VCBeat Eggshell Research Institute published the white paper “Empowering Primary Healthcare: 2017 White Paper on Innovation in Primary Healthcare,” the first industry report to provide a comprehensive overview of the primary healthcare sector.Conducted by eight researchers at VBInsight, this report is based on a four-month study of over 300 innovative companies in the primary healthcare sector. The reportThis article explores the development trends of the primary healthcare industry from the perspectives of industrial policy, technological evolution, business models, and industry collaboration, while also sharing more than 20 outstanding case studies of primary healthcare practices.
Leveraging the Internet and other technologies, new business models are emerging and expanding rapidly. Coupled with favorable policy reforms, this trend will significantly promote the two-way flow of high-quality medical resources. Patients, physicians, institutions, and regulators will all be empowered with new capabilities. As these early signs indicate, the primary healthcare industry is poised for a new wave of transformation!
We aim to address ten key issues in primary healthcare:
1. Why is the primary healthcare industry poised for a "golden decade"? How can stakeholders seize these industrial opportunities?
2. Why is the optimal entry point for the industry to “empower” primary healthcare?
3. How to empower primary healthcare? What are the four key empowerment directions, and what are the critical points within each?
4. Which empowerment direction is more challenging, and which offers the highest certainty of returns? What is the most rational development path?
5. What industrial chain opportunities does empowering primary healthcare bring?
6. What Are the Pitfalls and Misconceptions That Cannot Be Ignored in Empowering Primary Healthcare?
7. Which companies are empowering primary healthcare? Who are the best practice cases?
8. Should enterprises pursue deep regional penetration or rapid market expansion in their business development strategies for primary healthcare?
9. In terms of strategic direction, should we adopt full-chain empowerment or single-link empowerment?
10. What new opportunities will empowering grassroots healthcare bring to internet healthcare companies?
“Empowerment” is precisely the most important keyword that runs through this historic opportunity. Below is “Empowering Primary Healthcare — 2017 White Paper on Innovation in Primary Healthcare》Excerpt,See the end of this article for instructions on how to obtain the full white paper.。
1. Primary Healthcare Embraces New Development Opportunities
Policy-driven demand is shifting to the grassroots level; once successfully implemented, the primary care market will see an incremental opportunity worth RMB 500 billion.
In September 2015, the General Office of the State Council issued the “Guiding Opinions on Promoting the Construction of a Tiered Diagnosis and Treatment System,” which proposed assessment and evaluation criteria for pilot programs on tiered diagnosis and treatment. These criteria included achieving a proportion of at least 65% for visits to primary healthcare institutions out of the total number of medical visits by 2017. According to the “2016 Health and Family Planning Statistical Yearbook,” the number of visits to primary healthcare institutions nationwide in 2015 was 4.34 billion, accounting for 56.4% of the total number of medical visits, with an average outpatient cost per visit of RMB 97.7. If the proportion of visits to primary healthcare institutions were to reach 65% of the total, assuming the average outpatient cost per visit remained unchanged at the 2015 level of RMB 97.7, the annual outpatient expenditure at the primary care level would amount to RMB 488.7 billion. This figure would be even higher if inpatient costs incurred at primary healthcare institutions were included.
As the Spring River warms, “drugs” are the first to know: Medication growth at grassroots levels far outpaces that of large hospitals
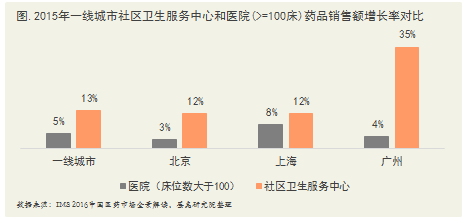
According to IMS Health’s “Panoramic Interpretation of China’s Pharmaceutical Market in 2016,” sales of pharmaceuticals in Chinese community healthcare settings reached RMB 42 billion in 2015. Among these, the sales growth rate at community health service centers in first-tier cities was 13%, significantly higher than that of hospital channels. Notably, Guangzhou saw a remarkable 35% increase in sales at its community health service centers, primarily attributed to the city’s implementation of a primary care-first diagnosis system. By adjusting reimbursement ratios across different levels of medical institutions, this policy substantially increased the proportion of initial consultations conducted at primary care facilities.
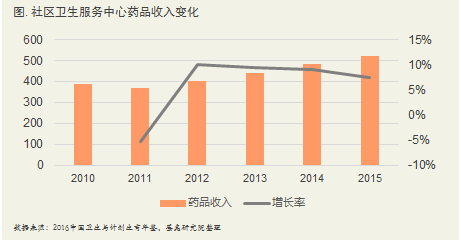
The proportion of drug revenue at the primary care level continues to rise, with overall drug revenue steadily increasing. According to the 2016 Yearbook of Health and Family Planning, the average drug revenue of community health service centers increased continuously from 2011 to 2015. The average drug revenue was RMB 3.881 million in 2010 and reached RMB 5.198 million in 2015, representing an average annual growth rate of 6%.
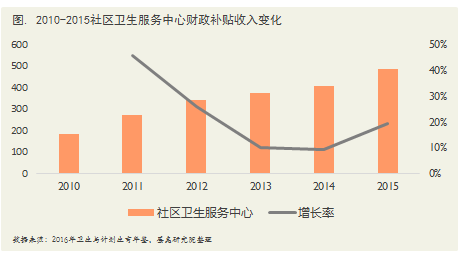
Average fiscal subsidy revenue for primary healthcare institutions has continued to rise. In 2010, the average fiscal subsidy revenue for community health service centers was RMB 1.852 million, which increased to RMB 4.878 million by 2015, representing an average annual growth rate of 21.3%. Additionally, the proportion of fiscal subsidies in total revenue has also been steadily increasing. Taking community health service centers as an example, the share of fiscal subsidies in their total revenue rose from 22.9% to 36.5%, indicating a significant change in their revenue structure.
Analysis of Key Healthcare Reform Tasks During the 13th Five-Year Plan Period—Clear and Definitive Top-Level Design
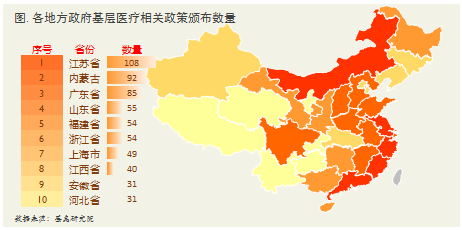
Development Opportunities in Primary Healthcare, Driven by China’s Continued Promotion of Tiered Diagnosis and TreatmentTracking of policies related to primary healthcare by VCBeat shows that tiered diagnosis and treatment has long moved beyond mere planning and top-level design. It has seen substantial acceleration across all aspects and is being comprehensively implemented throughout China. This progress is reflected not only in the increasing number of national policies issued for primary healthcare but also in the active implementation and promotion of these policies by various provinces and municipalities.
At the State Council executive meeting held at the end of 2016, key tasks for deepening healthcare reform during the “13th Five-Year Plan” period were determined.
Among the key tasks of healthcare reform, numerous initiatives are related to primary care, with the family doctor system prioritized as the most critical. In 2017, family doctor contract services were to be rolled out in more than 85% of prefecture-level cities, aiming for a family doctor service coverage rate of over 30%, and a contract service coverage rate of over 60% for priority populations. The policy not only outlined strategic directions but also established specific evaluation criteria. Achieving these targets will bring about transformative changes to China’s healthcare environment and service delivery models, while also creating new development opportunities for the internet healthcare industry. Regarding the implementation of tiered diagnosis and treatment, the state began promoting family doctor contract services in mid-2016. In addition to administrative measures to advance tiered diagnosis and treatment, economic incentives have been introduced, and many regions have liberalized licensing for private medical institutions.
At the national policy level, more than 50 policy documents have addressed primary healthcare annually over the past five years. Primary healthcare is a relatively broad concept, primarily encompassing primary healthcare institutions, primary care physicians, and patient utilization patterns at the primary care level. Key questions remain: How can primary healthcare be effectively advanced? How can patient visits be shifted downward to the primary care level? These objectives require gradual implementation. A breakdown of keywords related to primary healthcare reveals that early policy documents were predominantly overarching guidelines centered on “primary healthcare.” Over time, there has been a growing number of practical policy documents focused on operational mechanisms such as tiered diagnosis and treatment, telemedicine, family doctor services, and medical consortia, all aimed at promoting the decentralization of healthcare resources to the primary care level.
The establishment of a tiered diagnosis and treatment system aims to reverse the current unreasonable pattern of medical resource allocation, address the imbalance in resource distribution, guide residents to seek initial consultations at primary care institutions, and improve the efficiency of the healthcare system. Therefore, the most significant driver for strengthening primary healthcare is the implementation of tiered diagnosis and treatment. This trend is further evidenced by the year-on-year increase in the frequency of mentions of “tiered diagnosis and treatment” as a keyword.
Hierarchical Diagnosis and TreatmentThe so-called hierarchical diagnosis and treatment system involves classifying diseases based on their severity, urgency, and the complexity of required care, with medical institutions at different levels assuming responsibility for treating corresponding conditions. This tiered model, spanning from general practice screening to specialized treatment, aims to achieve initial consultations at primary care facilities, bidirectional patient referrals, differentiated management of acute and chronic conditions, and coordinated care across various levels of the healthcare system. Ultimately, it seeks to establish an ideal healthcare pattern where minor ailments are managed within the community, serious diseases are treated in hospitals, and rehabilitation takes place back in the community. Establishing a hierarchical diagnosis and treatment system is a complex systemic project with broad implications and intricate circumstances, requiring a long-term process to implement effectively.
The realization of tiered diagnosis and treatment requires a robust primary care foundation, necessitating the strengthening of all stakeholders involved in primary healthcare. Relevant policies for primary healthcare exert force from three angles: the supply side (medical institutions and physicians), the demand side (patients), and the payment side. Through policy-driven reinforcement, the primary healthcare system is being progressively improved.
Doctors—Weak Competence at the Primary Care Level, Outdated Equipment
China’s primary care sector suffers from a severe shortage of high-quality medical talent. The number of general practitioners is critically insufficient, and most have not undergone standardized residency training. Coupled with a lack of equipment, their clinical diagnostic and treatment capabilities are relatively weak. There is a significant gap between primary care physicians and hospital-based doctors in terms of educational background and professional titles. High-level physicians are scarce in primary care institutions; only 1.6% hold master’s degrees or higher, while the majority possess only secondary vocational or associate degrees. Consequently, misdiagnoses are prone to occur in routine clinical practice.
Medications — Limited Variety
On August 18, 2009, China officially promulgated the “Implementation Opinions on Establishing the National Essential Medicines System,” the “Administrative Measures for the National Essential Medicines List (Interim),” and the “National Essential Medicines List (Portion for Allocation and Use in Primary Healthcare Institutions)” (2009 Edition), marking the formal implementation of China’s efforts to establish the National Essential Medicines System.
Following the implementation of the Essential Medicines System, although the financial burden of medical expenses on the public has been alleviated to some extent, the narrowed drug formulary fails to meet the needs of special populations. In particular, chronic outpatients covered by the New Rural Cooperative Medical Scheme (NRCMS) have been unable to fully benefit from fixed subsidies or reimbursement policies due to drug shortages and established medication habits, leading to dissatisfaction with primary healthcare institutions. Key priorities for future healthcare reforms will include expanding the variety of essential medicines, improving service offerings at community health centers, enhancing medical technical capabilities, and ensuring smooth two-way referral channels within medical consortia.
Patients – Low Trust in and Awareness of Primary Care
Due to the combination of these factors, residents lack trust in primary healthcare institutions, making it difficult for them to retain patients. Driven by policy support and aided by new equipment and technologies, patients can enjoy higher reimbursement rates, more convenient diagnostic and treatment services, and equivalent clinical outcomes when receiving initial care at primary healthcare facilities. This approach encourages residents to seek care within their local communities and primary healthcare settings.
For a long time, the perceived bottleneck of healthcare reform has been the weakness of primary care institutions. The state has invested substantial human, material, and financial resources in an effort to establish a healthcare system featuring initial consultation at the primary level, two-way referrals, and tiered diagnosis and treatment.
Although achieving this goal presents numerous challenges, retreat is not an option; the issues facing primary care institutions are unavoidable hurdles that must be overcome. Addressing these problems and implementing a tiered diagnosis and treatment system represent the opportunities afforded to us by the market. How can we improve the service quality of primary care physicians? How can we standardize clinical protocols? How can we enhance mutual trust between doctors and patients? These are all significant challenges confronting primary care institutions.
Policy is the core driver behind the development of the primary healthcare industry. The main direction of policy guidance is to “empower” primary healthcare. But why exactly is empowerment necessary? Who are the recipients of this empowerment? How should it be implemented? Are there optimal pathways during the empowerment process, or potential pitfalls and misconceptions? What impact does empowering primary healthcare have on the entire health industry chain? In pursuing the empowerment of primary healthcare, should companies focus on deep cultivation or prioritize rapid expansion and market capture? Readers will find our reflections on these questions in the following text. We believe that our insights merely serve as a starting point; if they can inspire further thought and practical action among readers, then this report will have truly created value.
1. Building a New Ecosystem for Primary Healthcare, Seizing the Opportunity for Innovation in Medical Service Models
Primary Care Faces Numerous Long-Standing Pain Points, Urgently Requiring “Empowerment” of Its Service System
In recent years, to address the challenges of difficult and expensive access to medical care, the Chinese government has actively promoted various policy initiatives. Taking tiered diagnosis and treatment as an example, efforts have been made to establish a model featuring initial consultations at primary care institutions, two-way referrals, separate management of acute and chronic conditions, and coordination between different levels of healthcare providers. Under this policy guidance, provinces across the country have successively issued implementation plans for tiered diagnosis and treatment systems. However, the healthcare access issues faced by Chinese residents have not been alleviated, with patient flow still concentrating upward toward higher-level hospitals. Data comparisons from the *Statistical Yearbook of Health and Family Planning* in recent years show that the proportion of visits to primary care institutions remained low from 2009 to 2015, and these figures may even be overestimated. This is because local primary healthcare institutions often count various free public health services as “clinical consultations” to improve their performance evaluations. Despite national regulation and vigorous local implementation, the goal of initial consultations at the primary care level has not been achieved. The reason is clear: primary healthcare has failed to meet the needs of key stakeholders (primarily primary healthcare institutions, primary care physicians, and patients). Specifically, primary healthcare institutions still suffer from limited service capacity, primary care physicians have inadequate professional competence and insufficient motivation, and these factors have led to patient distrust and a weak willingness to seek initial care at the primary level, thereby trapping primary healthcare development in a vicious cycle.

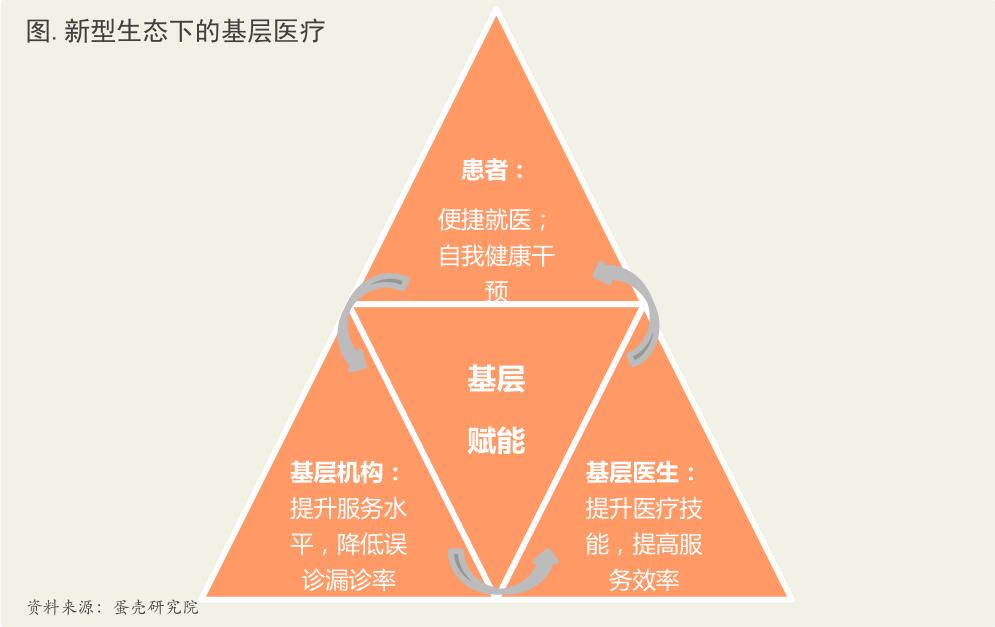
The current state of primary healthcare is characterized by widespread shortages: healthcare institutions lack talent, equipment, and operational capabilities; physicians face insufficient income, limited professional growth, and inadequate skills; patients suffer from a lack of trust, awareness, and respect. The key to empowerment lies in addressing the genuine needs of existing market participants in primary healthcare, with the fundamental goal of creating value for both consumers and payers. We believe that empowering healthcare institutions, physicians, patients, and regulatory authorities constitutes the four most critical directions for empowerment. The crucial point is to enhance the efficiency of empowerment, identify real problems, and provide precise support, thereby avoiding the “pitfalls of empowerment.”
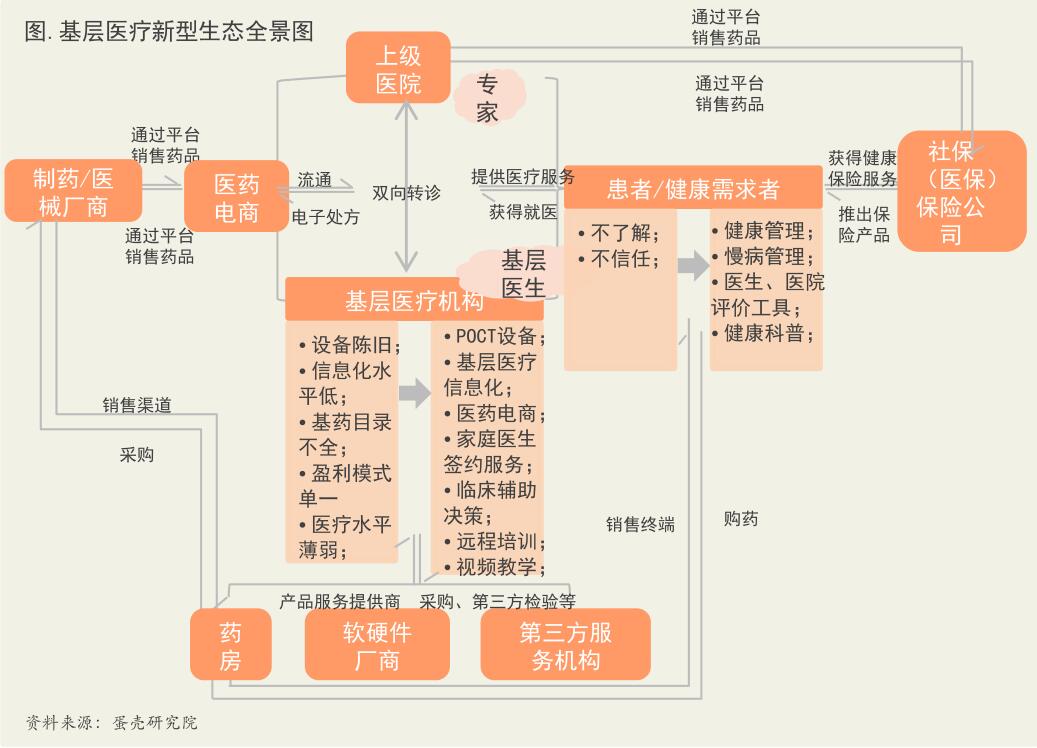
New Technologies and Business Models Rapidly Penetrate, Building a New Ecosystem
Amidst the impact of emerging trends such as mobile internet, artificial intelligence, big data, and the Internet of Things, a series of new technologies and models formed through cross-sector integration have gradually permeated every aspect of healthcare, particularly within the primary care service system, thereby establishing a new ecosystem for primary healthcare. This approach alleviates the challenges of "difficult and expensive access to medical care" through multiple dimensions, starting from surrounding communities and primary care levels, and adopting a bottom-up strategy. For instance, regional health information platforms have been established to enable community residents to access high-quality medical resources, facilitating interconnectivity, information sharing, and regional collaboration among hospitals, community health information service centers, and medical administrative departments. Additionally, a suite of medical skills training tools has been developed to enhance the competencies of primary care physicians, allowing them to train anytime and anywhere to rapidly improve their technical proficiency. Furthermore, internet-based tools have been introduced from the patient’s perspective to assist individuals in self-managing their diseases.
The Golden Decade of New Ecological Empowerment for Primary Healthcare
The market potential and opportunities in primary healthcare have always existed. However, most industry practitioners previously lacked a pain-point-oriented mindset, often initiating projects by relying solely on existing resources. Yet, zero-sum competition over existing assets and repeated, futile efforts cannot break through the established equilibrium of interests. The structural imbalance of “overcrowding at the top tier and underutilization at the grassroots level” remains unresolved. Issues such as talent shortages and outdated equipment in medical institutions, insufficient motivation and skills among physicians, and patients’ lack of trust and health education cannot be addressed merely by leveraging existing resources. Fortunately, we are now witnessing incremental growth—policy-driven, technological, capital, and business model innovations. We have found that the key point where all these incremental factors truly take effect can be summarized in two words: “empowerment.” Empowerment creates fertile ground and delivers essential nutrients. As we know, without soil, it is difficult to establish forests, let alone see flowers bloom along the paths. Empowerment brings fertile soil, trickling streams, and gentle sunshine to the land of primary healthcare.
We believe that institutional empowerment should take precedence, with physician empowerment proceeding in parallel. Patient empowerment and regulatory empowerment are built upon the former two; this sequence must not be disrupted. Primary healthcare institutions are the starting point of the entire logical chain. Improvements and empowerment across multiple dimensions—such as hardware equipment, informatization, operational mechanisms, and incentive structures—can attract high-quality medical talent, thereby creating the possibility of resolving patient doubts and distrust. In other words, if the empowerment of primary healthcare institutions is not completed, and one merely focuses on the subsequent areas of empowerment, the likelihood of failure is relatively high.Physician empowerment focuses on two aspects: efficiency empowerment and technical empowerment. Efficiency empowerment addresses the issue where physicians possess the necessary capabilities but lack the energy and time to cover the existing patient volume. We consider this a secondary step; prior to this, skills empowerment is paramount. Skills empowerment serves as the foundation, while efficiency empowerment enables subsequent scaled coverage. Skills empowerment includes long-term skills empowerment (primarily through various forms of training, including remote training). However, short-term empowerment may be more critical, mainly involving assisted diagnostic decision-making and the application of AI. Only by combining long-term and short-term approaches can the issue of physician empowerment be effectively resolved.Patient empowerment is the final step. Only after successfully implementing the first two steps—institutional and physician empowerment—can we gradually change patient awareness and habits through efficient patient promotion, education, and guidance. Regulatory empowerment runs throughout the entire process, but it is challenging to manage, given that the regulators ultimately oversee the service providers.
We believe that all segments of the healthcare industry chain—including pharmaceutical manufacturing, pharmaceutical distribution, medical devices, medical services, healthcare informatics, and internet healthcare—can identify their own opportunities and positioning within the major industrial trend of empowering primary care. Among these, the Direct-to-Patient (DTP) model in the pharmaceutical sector warrants attention. The integration of home delivery services in pharmaceutical distribution with primary care is likely to increase order density and average transaction value compared to previous models, thereby reversing the long-standing profitability challenges faced by pharmaceutical O2O platforms. Medical devices, including Point-of-Care Testing (POCT) and rehabilitation equipment, will benefit from the specialized roles assigned to chronic disease management and rehabilitation care at the primary level. High-end medical services and convenient medical services (including health management models) may also redefine their positioning amidst the new trends in primary care. Healthcare informatics presents a near-certain growth trajectory; however, due to the limited payment capacity of current payers, its profitability model may need to undergo certain transformations, shifting from a B2B model to a B2B2C or B2C model. Regarding internet healthcare, we believe that a consumer-review platform model (similar to Dianping) for primary care physicians and institutions will inevitably emerge and play a significant role. This will foster a virtuous cycle for primary care institutions and talent, thereby avoiding the adverse scenario where inferior providers drive out superior ones.
1) Empowering Primary Care Institutions – Enhancing Service Delivery Capabilities
Addressing the pain points of primary healthcare institutions, the primary objectives are to enhance medical service capabilities and reduce operational costs. This includes achieving accurate disease diagnosis through portable medical devices; advancing healthcare informatization by integrating new software systems to improve service quality and operational management efficiency at the grassroots level; and facilitating resource matching via platforms, thereby empowering institutions with diversified value. We believe that healthcare informatization, rapid diagnostic testing equipment, and rehabilitation devices constitute a proactive response to achieving the goals of primary healthcare institutions.

2) Empowering Primary Care Physicians—Enhancing Skills and Efficiency
Primary care physicians leverage “Internet+” products, services, and other solutions to enhance their clinical skills and work efficiency, thereby improving the quality of medical services. For instance, professional physician communities and clinical decision support tools provide career support and strengthen professional competencies. Additionally, web-based or mobile app platforms optimize healthcare service workflows, boosting service delivery efficiency.

3) Empowering Patients—Knowledge Empowerment
The core pain point for patients is a lack of trust, which essentially stems from insufficient understanding—both of their own medical conditions and of health insurance policies. By leveraging internet healthcare tools, patients can access desired health information in real time and consult with online physicians through platforms. This approach fully mobilizes medical resources, enabling services such as home visits by family doctors and allowing residents to receive medical and rehabilitation care without leaving their homes.

Overall, primary healthcare is in a period of industry growth. Driven by numerous factors such as technology and policy, we believe that teams with strong technical capabilities and clear business models are poised to become the leaders in reshaping the new ecosystem of primary healthcare. Within this effort to reshape the primary healthcare ecosystem, the government plays a leading role by formulating and issuing a series of relevant policies and regulations, providing financial support and other investments, and vigorously advancing comprehensive reforms of primary healthcare institutions, including township health centers and community health service organizations.
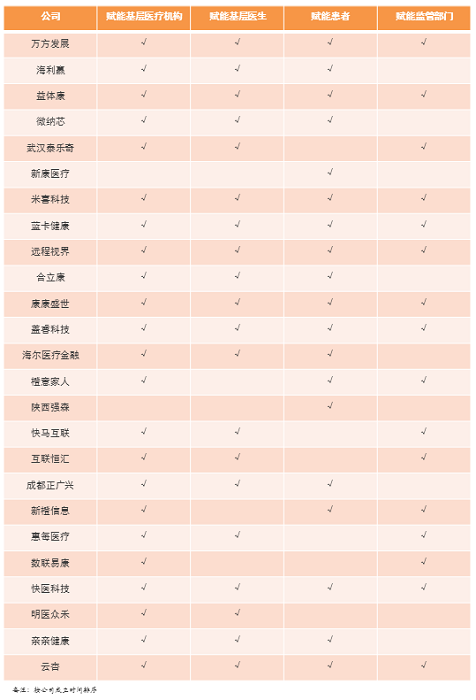
This section will discuss government regional samples and innovative practice cases separately. For the innovative practice cases, we selected 25 companies in China based on their approaches to resolving core issues and their model innovations, with the aim of providing insights for industry professionals and policymakers.
Chronic Disease Management Becomes the Most Reliable and Rewarding Revenue Stream for Primary Care.
The Golden Decade of New Ecological Empowerment for Grassroots Healthcare.
Service Capability – Efficiency and Skills – Knowledge: Four Major Directions Empowering Primary Healthcare.
Two Major Misconceptions and Pitfalls in Empowering Primary Healthcare.
Empowering Primary Healthcare Will Fully Drive Growth Across the Entire Big Health Industry Chain.
(The above is a partial excerpt from this report.)
This is China's first research report on innovative practices in primary healthcare—“2017 White Paper on Innovation in the Primary Healthcare Industry》, it examines policy orientation, pilot regions, primary healthcare institutions, technological breakthroughs and applications, and family doctors, thereby clarifying the development trajectory of China’s primary healthcare industry and presenting a comprehensive overview of its landscape.
Scan the QR code below to becomeVCBeat Official Member, you can obtain the full version《Empowering Primary Healthcare — 2017 White Paper on Innovation in Primary Healthcare》. Moreover, in the coming year, you will have unlimited access to the completeIndustry Trend Report, promptly grasp the latest globalInvestment and Financing Information, boasting a comprehensive range ofHealthcare Enterprise Database, and alsoMassive Resource Matchmaking。

Scan the QR code to become a VCBeat member,
Beta Version Trial Price: ¥365/year.