International Experiences in Primary Healthcare Workforce Development: Insights from Five Countries for Rural China

Professor Liu Xuanlin, School of Health Management and Education, Capital Medical University
From May 17 to 18, VCBeat’s “2017 China Primary Healthcare Innovation Practice Forum” was held in Chengdu. Professor Liu Xuanlin from the School of Health Management and Education at Capital Medical University delivered a presentation titled “International Experience and Implications for Rural Healthcare Workforce Development.”SubjectSpeech: This article presents an edited compilation of its highlights.
Guest Introduction
Liu Xuanlin
Graduate Supervisor at Capital Medical University, Executive Director of the Chinese Health Law Society, and Expert in the Guidance Group of the Department of Primary Health Care under the National Health and Family Planning Commission.
Key Highlights of the Speech
I. The Current State of Primary Healthcare in China: A Large Patient Population with a Shortage of Physicians, Facing a Long and Arduous Journey
II. International Explorations in Primary Care: The United States, Japan, Australia, Thailand, and South Africa
III. How to Innovate in the Future
I. Numerous Healthcare Institutions and Patients, Coupled with Staff Shortages
As of November 2016, the number of healthcare institutions in China had exceeded 990,000. Among these, there were more than 28,000 hospitals, accounting for 2.90% of the total, while primary healthcare institutions constituted the absolute majority, surpassing 93.81%. Sichuan Province ranked first among all 31 provinces and municipalities nationwide in terms of total healthcare resources, number of hospitals, and number of primary healthcare institutions.
Each year, the number of patient visits to various medical and healthcare service institutions in China continues to rise, albeit at varying rates. Patient visits to primary healthcare institutions have grown the most slowly, despite these facilities serving a substantial population with significant healthcare needs. Although there are over 10 million healthcare professionals nationwide, only more than 3.5 million of them work in primary healthcare institutions.
According to statistics from the National Bureau of Statistics, rural areas currently account for 94.7% of China’s total territory. This means that primary healthcare institutions, which constitute 93.81% of all medical and health institutions, possess only 34.56% of the total medical personnel yet are responsible for serving 94.70% of the rural population. It is evident that primary healthcare services are not only under significant pressure but also face a long and arduous journey ahead.
In primary healthcare, there are many examples closely related to internet-based medical services, such as telemedicine. In fact, most countries restrict telemedicine to follow-up visits (excluding initial consultations). However, in remote areas or other special circumstances, initial consultations are also permitted, constituting exceptions. This example illustrates, to some extent, that applying an urban efficiency-oriented mindset to address rural healthcare issues often leads to certain biases.
II. Insufficient Operational Capacity of Community Health Service Centers
Currently, the distribution of healthcare institutions in China is uneven, and there is a shortage of health human resources, particularly at the primary care level. Taking Beijing as an example, among the more than 3,400 administrative villages in its 10 remote suburban districts, over 900 are “blank villages” lacking basic medical services.
What Is a “Blank Village”? It refers to an entire administrative village that has neither a community health service station nor a village clinic. Data from surveys conducted over the past decade indicate that establishing stations under community health service centers can only address the issue in certain areas and lacks broad applicability for widespread adoption.
For example, a suburban district in Beijing piloted a program in one of its townships by deploying eight community health service stations, but ultimately recalled seven of them. The Community Health Service Center found that the operational and service capacities of the dispatched stations were inadequate, necessitating their eventual recall.
Primary healthcare service capacity is an issue that must be addressed. Why has primary healthcare service capacity failed to improve? The most prominent problem is the low professional appeal of primary healthcare services, and the enthusiasm and creativity of medical personnel have not been fully stimulated.
Therefore, the construction and sustainable development of the rural health service workforce will hinge on two critical aspects: talent cultivation and enhancing professional attractiveness. While a new type of medical and health workforce will inevitably emerge in rural areas in the future, an unavoidable question remains: where will primary healthcare professionals come from, and how should they be trained?
These issues are not unique to China. Other countries face similar challenges in the realm of primary care. Taking the United States as an example, although its healthcare institutions collectively provide comprehensive medical services, there is still a significant shortage of talent in rural primary care areas. Let us now examine their solutions.
United States: Four successive initiatives were implemented to strengthen primary healthcare capacity.
1. Physician Shortage Area Program
2. Rural Medical Education Program
3. Rural Medical Education and Implementation Development Project (Rural Education and Action Development)
4. Rural Physician Associate Program
The initial measure adopted in the United States was local selection, providing incentives for rural personnel. The second requirement is having a rural background and completing coursework in rural medicine. This is followed by field visits and internships in rural communities, as well as assigning mentors specializing in rural healthcare to medical personnel. In the United States, physician selection is highly rigorous, requiring first professional licensure and subsequently technical qualifications.
In addition, financial investment is equally indispensable, requiring support from dedicated funds; physicians must undergo general practice training before assuming their posts. While controlling scale, emphasis must also be placed on quality.
Japan: Joint Establishment of Jichi Medical University by Central and Local Governments
In Japan, the shortage of rural physicians is severe, with its physician-to-population ratio ranking near the bottom among the 30 OECD (Organisation for Economic Co-operation and Development) member countries.
Japan adopted a model in which the central government and local governments jointly established Jichi Medical University, with costs shared equally between the central government and 47 local prefectural governments. Meanwhile, these 47 local governments collectively contributed to a funding pool dedicated to university administration and student training. Each year, each region is allocated only two to three admission slots.
In other words, there are only about 100 spots available nationwide each year.
However, such a strategy is not realistic in China. This year, the Beijing Municipal Health and Family Planning Commission also established a primary care training program in collaboration with a university, with an expected enrollment of 300 students per class. Yet given China’s vast size, this translates to only about three trainees per district or county. It is worth noting that a single township typically comprises around 30 administrative villages.
This Japanese medical university implements a six-year training program, under which students are required to sign contracts committing to a nine-year service period. The college arranges for students to undertake clinical internships in rural areas to familiarize themselves with the rural working environment, followed by three years of residency training at general hospitals. Lastly, as the competent authority, the government oversees job placements and monitors compliance with these contractual obligations. In case of breach of contract, students must refund their educational expenses plus an annual interest charge of 10%.
Other countries: Australia, Thailand, South Africa
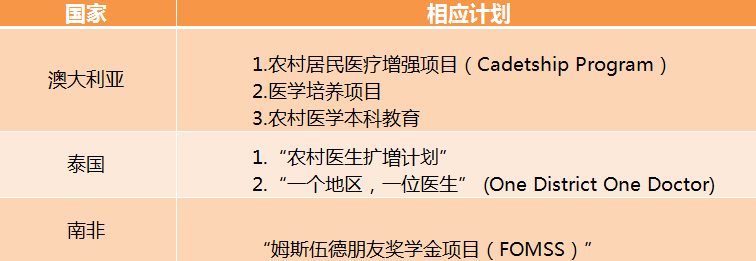
Other countries have their own realities, while China has its unique characteristics. How can China ensure that students acquire practical skills, are willing to work at the grassroots level, and remain in their positions? In recent years, many provinces have made efforts and launched pilot programs, primarily implementing the following three measures:
1. Implement order-based talent development programs (in provinces and municipalities such as Beijing, Shanxi, and Jiangsu) and strengthen project management and evaluation;
2. Increase financial investment to fulfill the government’s obligation to provide for citizens’ right to health;
3. Improve the compensation and benefits for grassroots medical personnel, innovate new working mechanisms, and enhance the profession's attractiveness.
Primary healthcare is further divided into three tiers. The lowest tier is the village level, which serves as the foundation of the network. Many internet-based medical services require integration with this tier, making it most challenging to determine who should deliver these services.
In urban areas, there are clear pathways for physicians to advance in professional title. However, the situation is different for rural doctors: there is little distinction between those who have practiced for a few years and those with decades of experience, as no corresponding promotion framework exists. This is inequitable.
Not only that, while medical staff in hospitals can have their liability for medical malpractice covered by medical liability insurance, rural doctors face a different reality. Once a medical malpractice incident occurs, they not only risk suspension of practice but may even face family bankruptcy, as many regions have yet to establish risk-sharing mechanisms for medical malpractice, such as medical liability insurance, compensation funds, and mutual aid funds.
Furthermore, the pension issue for rural doctors remains unresolved. Given their modest incomes, this group faces significant concerns about their future security. Although many provinces are moderately increasing rural doctors’ income through government-purchased services, subsidies for rural doctors across China actually range from only a few hundred to several thousand yuan, with some areas providing no subsidies at all.
If they struggle to make a living, how can these individuals dedicate themselves wholeheartedly to serving the healthcare industry, or undertake labor-intensive public health services such as chronic disease prevention and control?
Through the efforts of governments at all levels and other relevant entities, the primary healthcare environment will gradually improve. It is projected that by 2025, China’s primary healthcare workforce will see significant enhancement, which may also drive further growth in the internet healthcare sector.