Comprehensive Analysis of Medical Consortium Policies Across China's 32 Provinces and Municipalities: Clarifying Industry Trends
This year, medical consortiums across China are proceeding in an orderly manner.
However, medical consortiums are not a new concept. As early as the 1980s, nearly 1,000 types of medical collaboration alliances in various forms were established across eleven provinces and municipalities, including Beijing, Shanghai, and Zhejiang.
Following the new round of healthcare reform, medical consortia have once again come into the spotlight, emerging as a new model of healthcare reform and entrusted with significant responsibilities in the new era.
On April 23, the General Office of the State Council issued the “Guiding Opinions on Promoting the Construction and Development of Medical Consortia” (hereinafter uniformly referred to as “Medical Consortia”).The Opinion states that promoting the development of medical consortia is a crucial step and institutional innovation in deepening healthcare reform. It facilitates the adjustment and optimization of the structural layout of medical resources, promotes the shifting of focus and resources in healthcare services to the grassroots level, and enhances primary care capacity. Furthermore, it enables better vertical integration of medical resources, improves the overall efficiency of the healthcare service system, and supports the effective implementation of tiered diagnosis and treatment, thereby better meeting the public’s health needs.
By the end of June 2017, all provinces (autonomous regions and municipalities) were required to formulate work plans for advancing the development of medical consortia, specifying local targets and timelines; by the end of October 2017, all tertiary public hospitals were required to initiate the development of medical consortia.
By 2020, on the basis of summarizing pilot experiences, comprehensively advance the construction of medical consortiums and form a relatively complete policy system for medical consortiums. All secondary public hospitals and government-run primary healthcare institutions shall fully participate in medical consortiums.
Three days later, the National Medical Consortium Alliance, initiated by the China International Exchange and Promotive Association for Medical and Health Care and jointly participated in by one hundred hospitals and industrial institutions across China, was established in Shanghai.This is China's first open medical consortium platform jointly established by an industry association, medical institutions, and industrial organizations.
On May 24, the Sichuan Provincial Health and Family Planning Commission organized the drafting of the “Implementation Opinions on Promoting the Construction and Development of Medical Consortia (Draft for Comments).”. The draft opinion points out that,By 2020, a relatively comprehensive policy framework for medical consortiums will be established.
On the morning of May 26,Guo Hanwen, Director of the Medical, Health and Sports Committee of the Shaanxi Provincial Committee of the Chinese People's Political Consultative Conference (CPPCC), led some Standing Committee members and other leaders from the General Office of the Provincial CPPCC Committee,Conduct a Survey at the Red Cross Hospital, with a focus on the Red Cross HospitalOrthopedic Medical Consortium - Shaanxi Provincial Orthopedic Medical GroupConducted field research on the construction status and the implementation of remote consultations.
……
On June 5, according to the National Health and Family Planning Commission’s official website, the Joint Conference on Comprehensive Healthcare Reform for Shanghai, Jiangsu, Zhejiang, Anhui, and Fujian—comprising four provinces and one municipality—was held in Shanghai.In advancing the development of medical consortiums, Shanghai’s tertiary Grade A hospitals will serve as the leading entities, forming one or two medical consortiums with relevant healthcare institutions in Jiangsu, Zhejiang, Anhui, and Fujian provinces. Through the dissemination and outreach of high-quality medical resources, close collaboration will be carried out in disciplines, talent, technology, and management to enhance regional healthcare service capabilities.
According to official data from the National Health and Family Planning Commission, by the end of 2016, 205 prefecture-level and above cities across China had launched pilot programs for the establishment of medical consortiums, accounting for more than 60% of the total number of such cities.
What are the key policies governing medical consortiums across China? How have different regions established these consortiums, and what models have emerged? Have these medical consortiums truly optimized healthcare resource allocation by facilitating the downward transfer of physicians and technical expertise from large hospitals to primary care institutions? Have they resolved the persistent challenge of overcrowding in major hospitals while smaller facilities remain underutilized?
To this end, VCBeat (WeChat ID: vcbeat) has compiled medical consortium policies from across China to explore the resulting industrial opportunities.

2. The number of medical consortium policies issued annually has gradually increased
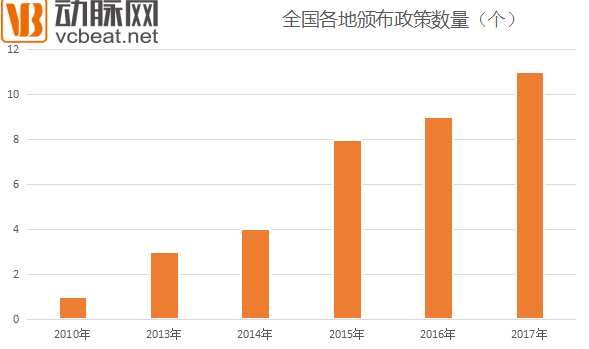
As shown in the chart, the number of policies related to medical consortiums issued across China has increased year by year. In particular, the number of policies promulgated in 2015, 2016, and 2017 was significantly higher than that in 2010, 2013, and 2014.
3. Numerous institutions across different regions participate in policy formulation
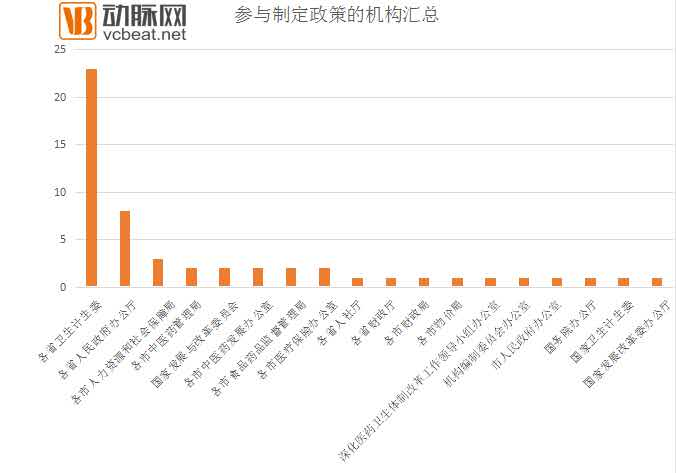
As indicated in the list, numerous institutions across China have participated in the formulation of medical consortium policies. These include the General Office of the State Council, the National Health and Family Planning Commission, the General Office of the National Development and Reform Commission, the National Development and Reform Commission, provincial health and family planning commissions, general offices of provincial people’s governments, provincial departments of human resources and social security, provincial finance departments, municipal bureaus of human resources and social security, provincial health and family planning commissions, municipal administrations of traditional Chinese medicine, municipal offices for the development of traditional Chinese medicine, municipal food and drug administrations, municipal medical insurance offices, municipal finance bureaus, municipal price bureaus, the Leading Group Office for Deepening the Reform of the Medical and Healthcare System, the Office of the Institutional Organization Committee, and municipal people’s government offices, among others.Among them, the provincial Health and Family Planning Commissions participated most frequently, followed by the General Offices of the Provincial People’s Governments and the municipal Human Resources and Social Security Bureaus.
4. Convergent Goals of Medical Consortia

From the perspective of listed objectives, Hainan Province and Shandong Province have set medical consortium development goals that are consistent with those proposed by the State Council, while other provinces have made corresponding adjustments.
5. Measures Implemented by Various Regions to Achieve Targets
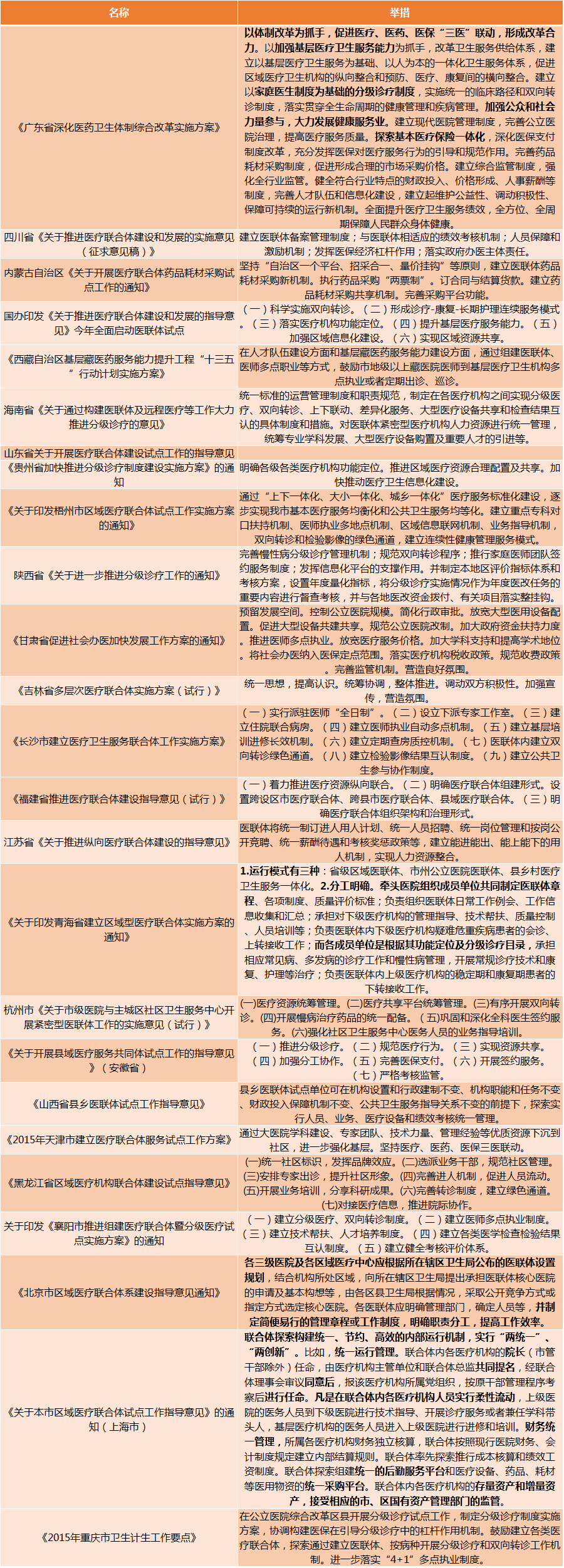
Based on the implementation of medical consortia across various regions, efforts have centered on establishing unified operational management systems and standardized responsibilities. Specific policies and measures have been formulated to achieve tiered diagnosis and treatment, two-way referrals, vertical coordination, differentiated services, sharing of large-scale medical equipment, and mutual recognition of test results among medical institutions. Human resources within tightly integrated medical institutions of the consortium are managed centrally, with coordinated planning for professional discipline development, procurement of large-scale medical equipment, and recruitment of key talent.
6. Four Models of Medical Consortiums
Medical Consortium refers to a regional medical alliance that integrates healthcare resources within the same area. It is typically composed of tertiary hospitals, secondary hospitals, community health centers, and village clinics within a region, forming a collaborative alliance or medical group that functions as a community of shared interests and responsibilities. The aim is to address the difficulty patients face in accessing medical care; for instance, minor ailments such as fever and colds can be treated at primary care facilities rather than overcrowding tertiary hospitals, thereby alleviating access barriers. This model achieves the intended goals of satisfying the public, the government, and healthcare workers.
From the perspective of the individual medical institutions that constitute a Medical Consortium, their modes of cooperation are categorized into two types: loose and tight. A tight-knit Medical Consortium is based on the integration of ownership and assets, forming an entity for service provision with shared financial responsibilities among the institutions. In contrast, a loose Medical Consortium is founded on the collaboration of elements such as technology, management, information, and payment systems, while asset ownership remains unchanged.
From the perspective of organizational models, medical consortiums can be categorized into four types. The first is the Urban Medical Group model. Led by tertiary public hospitals or hospitals with strong clinical capabilities, this model integrates community health service institutions and others to form a management framework characterized by resource sharing and division of labor. Within the medical consortium, cooperation is facilitated through mechanisms such as talent sharing, technical support, mutual recognition of examination results, prescription portability, and seamless service coordination.Represented by the Shenzhen Luohu Healthcare Group and the Jiangsu Zhenjiang Rehabilitation Medical Group.
For example, the Shenzhen Luohu Hospital Group consolidates district-owned public medical institutions in Luohu District, Shenzhen, under a single hospital group for unified management. It integrates multiple community health centers that were previously managed and operated by individual hospitals (“hospital-managed, hospital-operated”), leveraging the advantages of integrated group management to channel talent and resources down to the grassroots level.
Unlike the traditional public hospital groups, hospital alliances, and hospital consortia currently in China,The Luohu Hospital Group operates under a single legal entity, having fully integrated the Luohu District People’s Hospital, the District Hospital of Traditional Chinese Medicine, the District Maternal and Child Health Hospital, the District Rehabilitation Hospital, the District Geriatric Hospital for Integrated Medical and Elderly Care, and 48 community health centers into a unified hospital group for centralized management.
On the one handStrip away all the homogenized functions of public hospitals and integrate resources,Establishment of Nine Major Centers, Including the Clinical Laboratory Center and the Diagnostic Imaging Center, test results for patients can be shared and mutually recognized;On the other hand,,Implement Differentiated Development, taking the three major public hospitals in the current jurisdiction as examples, Luohu People's Hospital will focus on critical and complex cases in the future, the core development areas of Luohu Traditional Chinese Medicine Hospital are TCM, orthopedics, and rehabilitation, while Luohu Maternity and Child Healthcare Hospital will continue to leverage its traditional strengths. In addition, physicians can move freely among the hospitals within the group.
At the same time, was also establishedCommunity Health Service Management Center, handing over the community health centers in the region, which were previously affiliated with various medical institutions, to a single“Grand Steward”: Unified planning, unified standards, unified functions, unified operations, and integrated management.
According to reports, the newly established Luohu Community Health Management Center has restructured community health services into a three-tier system, with one regional community health center established in each sub-district.Each regional center provides synchronized guidance to three or four second-tier community health centers (equivalent to community health service stations), with third-tier self-service health management kiosks, thereby achieving the integration of community healthcare resources.
The second is the county-level medical consortium model.County-township integrated management, with county-level hospitals as the lead, township health centers as the hub, and village clinics as the foundation, effectively interfaces with village-township integration to establish a mechanism for division of labor and collaboration among the three tiers of medical and health institutions at the county, township, and village levels.
Represented by Tianchang, Anhui.Disorderly healthcare-seeking behavior at the county level has long been a prominent issue. To address this problem fundamentally, Tianchang City established a county-level medical consortium, transforming the previous competitive landscape in which medical institutions operated independently and vied for patients.
This is mainly achieved through the “Three Integrations,” “Three Principles,” and “Three Key Focus Areas,” which involve integrating urban and rural medical institutions, regional information platforms, and healthcare service resources.
Within the medical consortium, human resources, finances, and materials are managed centrally, with shared use of large-scale medical equipment. County-level hospitals partner with primary healthcare institutions to establish county-wide medical consortia. This facilitates information interoperability and remote consultation collaboration within the consortium, promoting the vertical flow of high-quality medical resources.
Adhere to the principle of shared benefits and implement capitation-based global prepayment; adhere to the principle of shared responsibility and establish a mechanism for division of labor and collaboration; adhere to the principle of aligned development and establish a mechanism for coordinated growth.
The third is the cross-regional specialty alliance.Supported by the specialized technical strengths of distinctive clinical departments in medical institutions, this approach fully leverages the roles of medical centers, clinical medicine research centers, and their collaborative networks. By fostering inter-specialty collaboration as a linking mechanism, it establishes a complementary development model to enhance disease treatment capabilities.
Represented by the Pediatric Alliance of Beijing Children's Hospital.Beijing Children’s Hospital has chosen to establish strategic alliances with provincial-level children’s hospitals, while requiring that members within the alliance form a province-wide medical consortium in their respective provinces. Provincial children’s hospitals drive municipal-level institutions, and municipal children’s hospitals in turn engage county-level and community hospitals. Through performance evaluations, if indicators such as the retention of common and frequently occurring diseases at the primary care level fail to show improvement, the institution may be removed from the group in the following year. The group has enhanced the comprehensive capabilities of its member hospitals by conducting academic exchanges, building research platforms, implementing co-developed departments, providing remote consultations, and dispatching expert teams for touring diagnoses and surgeries across various regions. Currently, a coordinated service model has been established, featuring “initial diagnosis at the primary care level, remote consultations for complex cases, and barrier-free referral for patients with difficult, critical, or emergency conditions.”
The fourth is the telemedicine collaboration network. Public hospitals provide telemedicine, remote teaching, and remote training services to grassroots, remote, and underdeveloped areas, leveraging information technology to promote the vertical flow of resources, enhance the accessibility of high-quality medical resources, and improve the overall efficiency of medical services.
Represented by the China-Japan Friendship Hospital Telemedicine Network.Through the telemedicine information management platform, unified management and application of systems such as software-based video remote consultations, high-definition video terminal consultations, 3D surgical remote teaching live broadcasts, and remote education and training are achieved, utilizing various access methods including digital dedicated lines, international VPN connections, and the Internet. A wide range of telemedicine activities have been conducted, including clinical consultations, imaging consultations, pathology consultations, teaching and training, 3D surgical demonstrations, multidisciplinary case discussions and ward rounds, and academic conferences.
Currently, although medical consortia have proliferated widely, the debate over which type of medical consortium is superior has never ceased.Liang Wannian, Director of the Department of System Reform under the National Health and Family Planning Commission, stated, “In the long run, if the division of labor among medical institutions within medical consortia is clearly defined, their roles are well-positioned, and assessment and evaluation mechanisms adapted to medical consortia are established, the effectiveness of tightly-knit medical consortia will be enhanced.”
“Currently, we encourage the development of close-knit medical consortia without imposing mandatory requirements, allowing for diverse models,” he added. The most important principle in building medical consortia is to shift the focus from emphasizing the efficiency of individual medical institutions to highlighting the overall efficiency of the entire healthcare service system.