Seven Strategies Top Hospitals Use to Control Pharmaceutical Costs
According to a research report released by the Blue Cross Blue Shield Association, although the United States has attempted to mitigate the impact of rising drug prices by emphasizing the use of generic drugs, this measure remains insufficient to curb the rapid increase in prescription drug prices in the country.
Currently, more than 80% of prescriptions are written using generic drug names; however, the prices of brand-name and specialty drugs continue to rise rapidly, with increases substantial enough to offset the cost savings achieved between 2010 and 2016.

Between 2010 and 2016, the annual price increase for drugs protected by patents and lacking generic competitors exceeded 25%, more than double the overall rate of drug price inflation. These drugs currently account for 63% of total U.S. pharmaceutical spending, up from just 29% in 2010. Furthermore, according to the report’s authors, “this upward trend shows no signs of abating.”
So, in the face of such rapid price increases, how should corporate employers and health insurers respond? VCBeat (WeChat: vcbeat) takes three U.S. healthcare institutions—Cleveland Clinic, Cedars-Sinai Medical Center, and Wexner Medical Center—as examples to briefly outline and introduce several strategies for controlling drug costs.
Cleveland Clinic recently announcedFollowing the announcement of the drug cost-control plan, Jeff Rosner, Senior Director of Pharmaceutical Procurement, expressed skepticism. Given his deep understanding of the pharmaceutical market, he doubts whether Cleveland’s initiative will achieve its intended outcome—namely, effectively reducing high medication costs.

Cleveland Clinic
Jeff’s skepticism is well-founded, as hospitals and healthcare systems often have very limited leverage to control rising drug prices. It is difficult for hospitals to alleviate this financial pressure on their own.Particularly for inpatient care, the reimbursement coverage under medical insurance is significantly lower than the actual cost of medications.。
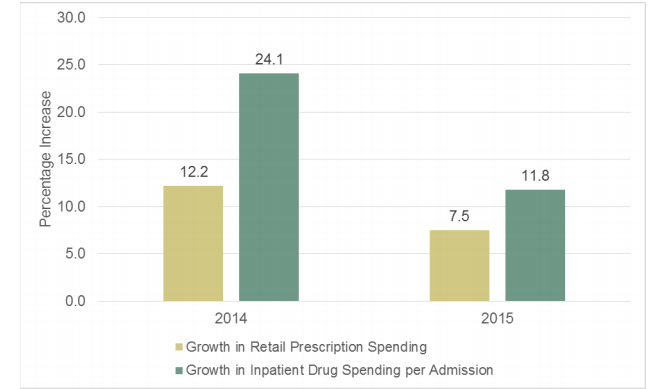
Comparison of Drug Cost Growth Between Inpatient and Retail Sectors, with Yellow Representing the Retail Sector and Green Representing the Inpatient Sector.
Despite numerous challenges, Cleveland Clinic successfully controlled medication costs without compromising the quality of care, saving a total of $90 million between 2010 and 2016.
Jeff gladly admitted, “I underestimated the impact of this initiative.” Of the $90 million saved, approximately 45% was achieved through inpatient services.The primary approach involves strengthening traditional medication management practices, such as implementing inventory control, prescription management, procurement, and medication use review.。
Although the aforementioned practices are not novel, Cleveland’s rigorous implementation and high level of prioritization have been key to achieving its goals. This success has also been facilitated by emerging information technologies, which provide classified data on drugs and drug categories to support cost-control efforts.
Direction 1: Prescribe according to actual conditions
Cedars-Sinai Medical Center is located in Los Angeles. There, physicians and pharmacists meet regularly to discuss the “gray areas” of medication use (a term coined by Chief Pharmacy Officer Rita Shane).
“We do not interfere with physicians’ decisions that benefit patients,” said Rita. “We only step in when there is ambiguity in medication selection, such as in gray areas where the optimal choice is unclear, when high-cost drugs may be required, or when lower-cost alternatives with equivalent efficacy and safety profiles are available. In such cases, we collaborate with physicians to determine the appropriate prescription for each specific case.”

Cedars-Sinai Medical Center
At the monthly Medication Use Policy Committee meeting at Cedars-Sinai Medical Center,The policy-making panel comprehensively evaluates factors such as the safety, efficacy, and price of various medications to determine whether adjustments are needed to the hospital’s formulary, recommended drug list, and medication policies.. Pharmacists will extensively collect information on the medications under review and share the obtained data with other healthcare professionals. Subsequently, this information will be submitted to the Pharmacy and Therapeutics Committee for final review.

Member of the Medication Policy Development Committee at Cleveland Clinic
In practice, it is difficult to obtain objective, neutral, and accurate information on various pharmaceuticals, as there are few comparative studies on the efficacy of different drug classes.
Len Gray, Deputy Director of the Clinical Services Department within the Comprehensive Pharmacy Services medical system, stated, “Most of the drug information we can access comes from the companies that sell these drugs. Only when we are able to obtain objective and reliable drug information, rather than just the marketing materials currently available, will we be able to make truly accurate judgments regarding drug efficacy and medication selection.”
To address this issue, pharmacists at Cedars-Sinai assign reliability ratings to retrieved drug studies. For instance, studies conducted in a randomized controlled manner can be rated as the highest level IA or IB, whereas reports provided by expert committees or anecdotal experiences from authorities are classified only as the lowest level IV.
In response, Rita stated, “After we share this information with the Pharmacy and Therapeutics Committee, the committee members will make decisions regarding the use and administration of these medications.”
For example,The committee may recommend imposing restrictions on patients using a specific medication, including limitations on the duration of therapy and the necessity of oral versus injectable administration.If high-priced drugs are neither safer nor more effective than lower-priced alternatives, the committee will remove them from the formulary. Of course, for special cases, physicians may still request to prescribe excluded medications, but only after consulting with a pharmacist.
Cleveland Clinic’s medication use review process is similar to that of Cedars-Sinai. Meghan Lehmann from the Drug Information Services department stated, “We add certain medications to the electronic health record (EHR) system to impose restrictions on their use. Specifically, when a physician prescribes a medication, a pop-up window appears in the EHR system to alert the physician that the prescribed drug is contraindicated for certain patient populations. The system also includes alert windows for pharmacists, prompting them to verify prescriptions containing restricted medications issued by physicians.”
For hospitals, a key challenge in implementing drug cost control lies in the necessity to monitor drug price increases in real time, yet such price hikes are often unpredictable.
To this end, the Cleveland Clinic has developed a data analytics tool that alerts pharmaceutical stakeholders to fluctuations in drug price peaks, facilitating their collaboration with physicians to rapidly identify lower-cost alternatives.
According to Jeff, “The tool can deliver analytical results in just 24 hours (at most 48 hours). Previously, obtaining information on drug price fluctuations required personnel to manually sift through extensive spreadsheets and databases.”
This tool searches for drugs with price increases by browsing drug catalogs automatically obtained from wholesalers. It also calculates the impact of this price increase based on the annual usage volume of a specific drug at Cleveland Clinic.Financial Impact on Hospitals. For instance, the tool recently alerted physicians in Cleveland that a price increase for lidocaine would incur an additional annual cost of $250,000 for the hospital, underscoring the importance of adjusting formularies.
Direction 2: Purchase Drugs Directly from Manufacturers
Applying for bulk purchase discounts is another major strategy for controlling drug costs. The conventional process for drug procurement involves pharmacists collaborating with physicians to select the drugs that the hospital will purchase from the available options within each therapeutic category. Subsequently, the hospital applies for discounts on the selected drugs, typically through group purchasing organizations (GPOs), which negotiate with pharmaceutical manufacturers on behalf of the hospitals to determine the discount rates.
Cleveland has adjusted this traditional process by directly engaging with pharmaceutical manufacturers.Jeff explained, “We negotiate the majority of our procurement contracts independently. While discounts are offered by pharmaceutical manufacturers, our first step is to determine which medications we intend to purchase. Our pharmacy team collaborates with physicians to validate the efficacy and safety of specific drugs through clinical outcomes. Once validated, they inform our procurement team, who then assess what level of discount can be secured from the manufacturer for that particular drug.”
Scott Knoer, Chief Pharmacy Officer at Cleveland Clinic, stated: “The key to our successful commercial negotiations lies in our drug formulary determination process and the integration of restricted medications into the electronic health record (EHR) system. We have established strong credibility because our physicians are involved in the drug decision-making process, and we incorporate the results of medication screening into the EHR system.”
Direction 3: Reduce Inventory
After clearing out unused, duplicate, and low-utilization medications from its warehouse, The Ohio State University Wexner Medical Center in Columbus, Ohio, reduced its drug inventory by $800,000 within one year.
This cost-control achievement is primarily attributed to the strict management of automated dispensing cabinets in nursing units.Robert Weber, a pharmaceutical services manager, stated, “Hospitals typically do not devote attention to these medication cabinets, nor do they regularly clear out unused medications.”

Wexner Medical Center
The key to pharmaceutical inventory management lies in maintaining a delicate balance. Robert stated, “We do not want to hold excessive inventory, but we must maintain sufficient stock to meet patient demand.” Strict control over pharmaceutical inventory can reduce hospital spending on unused medications and simultaneously decrease the volume of unused, expired drugs.
Another effective strategy is called “extending shelf life.” Robert stated, “We collaborate with an analytical laboratory to test the stability of certain medications and then decide whether to extend their shelf life based on the test results.” In fact, merely extending the shelf life of two drugs (clindamycin and remifentanil) has already helped Wexner Medical Center save $50,000 annually.
Furthermore, Wexner Medical Center has established a partnership with a consignment provider to implement on-demand ordering for certain high-cost, low-demand medications, rather than maintaining large stockpiles. For instance, by procuring subcutaneous treprostinil, used to treat pulmonary hypertension, through this on-demand model from the consignment provider, Wexner Medical Center saves approximately $140,000 annually.
According to Marvin Finnefrock, Director of Clinical and Procurement Services at Comprehensive Pharmacy Services: “These consignment providers help hospitals share part of the risk. They purchase and stock certain medications in advance, charging hospitals only when actual orders are placed.”
Many medication dispensing cabinets have achieved automated inventory management. Erin Fox, Director of Medication Information Services at University of Utah Health, stated, “Some cabinets monitor and report the number of medication bottles on the conveyor belt. Once the standard quantity is reached or reorder criteria are met, the cabinet automatically sends a restocking order to the wholesaler.”
However, from Erin’s user experience perspective, the interoperability of these inventory systems is poor. “Communication between systems is suboptimal, so each medication change requires significant manual effort. We have calculated that a single medication update necessitates reconfiguration across 17 different pharmaceutical inventory systems.”
To help staff keep abreast of pharmaceutical supply dynamics, Wexner Medical Center will deploy an inventory management module within its electronic health record (EHR) system this fall. This module will automatically provide alerts on the utilization of various medications across the hospital, facilitating the accurate setting of minimum inventory levels.
Direction 4: Expanding the Supply of Information Required for Decision-Making
Robert stated, “Prescription writing is the most effective way to influence physicians’ decision-making.” To fully leverage this opportunity, Wexner Medical Center added a price alert module to its electronic health record (EHR) system, which visually displays the price levels of different antibiotics. For instance, if the daily cost of an antibiotic is less than $1, a single cent symbol appears next to the drug name; if the daily cost exceeds $400, seven dollar signs are displayed beside it.
Furthermore, at Wexner Medical Center, pharmacists are integral members of the healthcare team. They directly participate in decision-making and medication selection processes, a practice that effectively prevents medication errors and reduces costs.
After University of Utah Health assigned a pharmacist to join the medical team, the resulting savings on medication costs were two to three times the pharmacist’s salary. Erin stated, “No one understands better than pharmacists how to effectively reduce drug costs while ensuring therapeutic needs and outcomes are met. Although adding a pharmacist to the medical team increases personnel expenses, this investment has proven to yield a very high return!”
Direction 5: Trends in Inpatient Medication Cost Changes
In recent years, “skyrocketing drug prices” have frequently made headlines in media reports. The price of epinephrine auto-injectors (EpiPens) surged from $100 to $600, representing a 500% increase. The cost of Sovaldi, the so-called “miracle drug” for hepatitis C, reaches as high as $84,000 for a 12-week course of treatment.
So, who is footing the bill for rising drug prices? The reality is complex, with significant differences between inpatient and outpatient settings. Typically, medication costs for outpatients are reimbursed by health insurance providers such as Medicare based on actual prescriptions, with patients only responsible for a portion of the cost; the out-of-pocket share varies depending on the type of insurance coverage.
However, the situation for inpatients is different. Medicare and other insurance payers typically reimburse hospitals a fixed amount to subsidize costs beyond direct patient treatment, including medication expenses. Yet, according to a 2016 joint report by the American Hospital Association and the Federation of American Hospitals titled "Trends in Inpatient Drug Costs: Issues and Challenges," this fixed payment falls far short of covering hospitals’ expenditures on medications for inpatients.
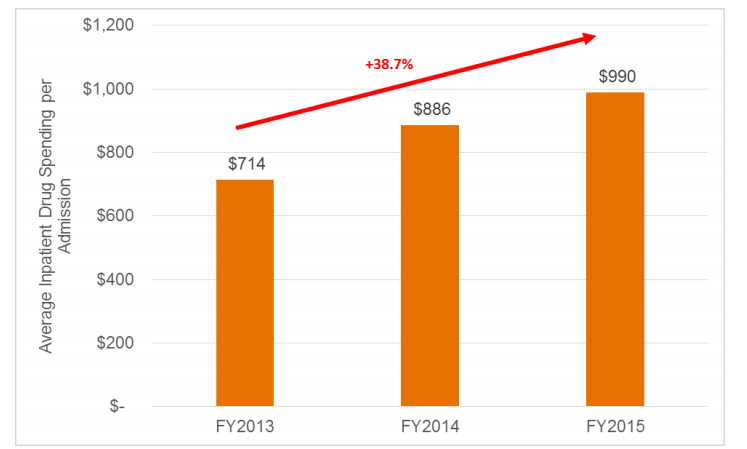
Average Drug Cost per Inpatient Case
Finally, to summarize. Overall, there are seven specific methods for controlling drug costs:
1. Uncover the "Gray Areas"
Review the medication list to identify any ambiguous areas, verify the necessity of high-cost drug usage, and confirm whether there are lower-cost alternatives with comparable efficacy and safety.
2. Monitor trends in drug price increases
Develop data analytics tools to alert pharmacists to drug price peaks, facilitating rapid identification of lower-cost alternatives in collaboration with physicians. Ideally, these tools should include functionality to calculate the financial impact of price increases on hospitals based on annual usage volumes.
3. Apply for Discount
Pharmacists and physicians jointly determine the hospital's drug formulary, and then apply for price discounts from pharmaceutical manufacturers through group purchasing organizations (GPOs) or independently.
4. Inventory Management
Implement strict controls over automated dispensing cabinets in nursing units. Promptly remove unused, duplicate, and low-utilization medications.
5. Extended Shelf Life
Collaborate with the Analytical Research Laboratory to assess the stability of certain pharmaceuticals and determine whether to extend their shelf life based on the test results.
6. Establishing Partnerships with Custodial Institutions
Identify high-cost, low-utilization medications and partner with third-party logistics providers to implement on-demand procurement without maintaining inventory.
7. Display drug price levels in electronic medical records to support decision-making
Implement a price-level alert module within the electronic medical record (EMR) system to automatically display comparable medications and their price tiers during prescription ordering, thereby facilitating informed clinical decisions that balance efficacy, safety, and cost.
Note: The above content is compiled. VCBeat strives to ensure the accuracy of the translation.
References:
http://www.hhnmag.com/articles/8271-hospitals-rein-in-inpatient-drug-costs
https://www.ptcommunity.com/news/20170612/how-cleveland-clinic-saved-90-million-drug-costs
https://mibiz.com/item/24866-analysis-finds-escalating-specialty-drug-costs-more-than-offset-savings-from-generics
http://www.hhnmag.com/articles/7732-new-aha-sponsored-report-details-how-drug-prices-are-crippling-hospitals-patients