From Medical Consortium to Physician and Healthcare Groups: A 15-Year Development Journey of West China Hospital
“West China Hospital must never become a pariah shunned by all,” said Huang Yong, Deputy Secretary of the Party Committee of West China Hospital, Sichuan University, in an interview with VCBeat (WeChat ID: vcbeat).
Elephants are currently the largest mammals on land and a symbol of strength. Although West China Hospital is located in Wuhou District, Chengdu, Sichuan Province, it has earned widespread acclaim both domestically and internationally, receiving countless awards, standing out as the strongest among the strong.
Historically, West China Hospital carries the genetic imprint of an international educational background, tracing its origins to Christian missionary societies from the United States, Canada, the United Kingdom, and other countries. In 1892, Renji Hospital and Cunren Hospital were established in Chengdu. In 1937, with the full-scale outbreak of the War of Resistance Against Japanese Aggression, National Central University, Yenching University, Cheeloo University, Jinling University, and Ginling Women’s College relocated to Chengdu, where they collaborated with West China Union University in education and medical services. In 1938, West China Union University (which had a medical school), National Central University, and Cheeloo University jointly established a united hospital. In 1946, the West China Union University Hospital was fully completed at its current location, abbreviated as West China Hospital.
It is a national-level center for the diagnosis and treatment of complex, critical, and severe diseases in Western China, as well as the world’s largest single-site general hospital. It houses China’s largest medical laboratory center, which was the first to achieve comprehensive accreditation from the College of American Pathologists (CAP).
West China Hospital comprises five campuses, with a total gross floor area of 485,300 square meters and a total authorized bed capacity of 4,300. It houses 44 clinical departments and 9 medical technology departments. The hospital operates its main campus on Guoxue Alley in Chengdu and the Wenjiang Medical Campus, and fully manages Chengdu Shangjin Nanfu Hospital (hereinafter referred to as “Shangjin Branch”). Each campus has a clearly defined service role: the main campus, with 4,100 beds, focuses primarily on the diagnosis and treatment of complex, critical, and severe conditions; the Wenjiang Campus, with 200 beds, specializes in rehabilitation, oncology, and chronic disease management.
Compared with other Grade 3A hospitals, West China Hospital is a true powerhouse. This status enables it to attract more high-quality medical professionals and patients; however, the original mission of the healthcare industry is to help as many people as possible. What measures has West China Hospital taken to break the monopoly on medical resources? How has it performed in the development of medical consortiums?
West China Hospital ranked first nationwide in the overall score on the 2015 Social Contribution Ranking of Public Hospitals in China. On Fudan University’s Rankings of Best Specialist Reputations and Best Hospitals in China, it has been ranked second nationwide for five consecutive years. For many consecutive years, it has been selected by independent third-party surveys as one of the top ten “Most Popular Grade-A Tertiary Hospitals Nationwide” and one of the top ten “Best Employers among Healthcare Institutions.”

In terms of academic papers and disciplines, West China Hospital had a total of 1,100 papers indexed by SCI in 2014, which increased significantly to 1,229 in 2016.
With its high-quality medical resources, West China Hospital not only serves the entire western region of China but also attracts numerous patients from both domestic and international locations.
According to Huang Yong, statistical data from West China Hospital over the past two years indicate that patients come from both domestic and international locations. Among domestic patients, 20% are from outside Sichuan Province, 40% are from within Chengdu, and 40% are from other parts of Sichuan Province outside Chengdu. The number of international patients is also increasing year by year, with individuals coming from more than 10 countries, such as Singapore.
“Although the number of patients is increasing, the bed capacity at the main campus of West China Hospital is limited and insufficient, leading to a severe issue of adding extra beds.” Huang Yong also expressed his helplessness regarding this situation.
Based on the categories of patient visits, West China Hospital recorded a total of 5.3 million emergency department visits, 220,000 discharges, and over 143,000 surgeries in 2016, with an average length of stay of 9.32 days and a day-surgery proportion reaching 24%. Evidently, the hospital’s outpatient clinics, emergency department, inpatient wards, and operating rooms are all operating at full capacity.
The resulting outcomes include a decline in the quality of medical services, strained doctor-patient relationships, and poor patient care experiences. On the other hand, during the 13th Five-Year Plan period, the focus shifted from medical treatment to health promotion, advocating for a tiered diagnosis and treatment system.
What Challenges Do Large Hospitals Face, and How Should They Develop?
Huang Yong believes that the challenges encountered in this process mainly come from three aspects:
First, supply-side reform has brought new challenges to the reform of public hospitals. The reform of urban public hospitals aims to resolve contradictions in their systems and mechanisms; the establishment of a tiered diagnosis and treatment system is intended to correct distortions in resource allocation.
Second, the expansion of the connotation and extension of social service demands poses challenges to such hospitals;
Third, technological advancements have brought new challenges and opportunities to the transformation of healthcare service models.
“Whether it is the reform of public hospitals or the establishment of a tiered diagnosis and treatment system, both have created a forcing mechanism for the operation and development of public hospitals. If they do not take the initiative to reform, the development path available to public hospitals may become increasingly narrow in the future.” Huang Yong is firmly convinced of this.
West China Hospital’s reform focuses on the “Three-Medical Linkage” (health insurance, pharmaceuticals, and public hospital reforms). The solutions can be succinctly summarized as “Dismantle, Establish, and Stimulate”: dismantling profit-driven mechanisms, establishing a modern hospital management system and a tiered diagnosis and treatment system, and stimulating hospitals’ initiative and creativity.
“While we have lost the ability to generate operational surpluses, physicians are now permitted to practice at multiple institutions. Within this broader policy landscape, the monopoly that hospitals once held over resources has been broken. The core challenge facing all large public hospitals is determining how to cultivate a culture that can retain high-quality talent and stimulate their enthusiasm and creativity,” said Huang Yong.
With the advancement of tiered diagnosis and treatment, the following issues may arise: first, ambiguous positioning of tiers; second, insufficient capacity at the primary care level; third, tiering without coordination, resulting in a lack of service continuity and disordered patient flow; fourth, patient experience; fifth, payment mechanisms; and sixth, administrative directives.
According to the documents issued by the State Council on medical alliances, there are four models of medical alliances promoted at the national level: Medical Consortiums, Medical Communities, Specialty Alliances, and Telemedicine Collaboration Networks.
“I believe that the Guidelines implicitly refer to two additional forms of medical consortia: urban and rural. In other words, rural tertiary hospitals are encouraged to take the lead in establishing medical consortia by taking over the management of county-level hospitals within their regions and forming medical groups, among other models. Meanwhile, in addition to local medical consortia, national and provincial hospitals may extend their reach across regions to collaborate with multiple medical consortia,” added Huang Yong.
Meanwhile, the state also encourages the development of closely integrated medical consortia, adhering to the principles of “Three Unchanged,” “Three Shared,” and “Three Unified.” The “Three Unchanged” refer to: unchanged asset ownership, unchanged channels for fiscal appropriations, and unchanged employee status. The “Three Shared” refer to: shared resources, shared talent, and shared information. The “Three Unified” refer to: unified internal management, unified resource allocation, and unified information platforms.
In fact, West China Hospital had already been implementing medical consortiums more than a decade before the state issued policies to vigorously promote their development.
“We have been engaged in this field for over a decade, experiencing both hardships and the joy of numerous achievements. More than ten years later, the national government began to advocate for the establishment of collaborative healthcare systems. Throughout our practical implementation, we have explored five models of medical consortia,” said Huang Yong.
According to Huang Yong, West China Hospital first initiated its medical consortium in 2002, when it proposed the establishment of a regional medical ecosystem. From 2002 to 2013, the hospital built a patient-oriented ecosystem, aiming to create a win-win situation for both healthcare institutions and patients. The following outlines the architecture of the entire regional medical system:
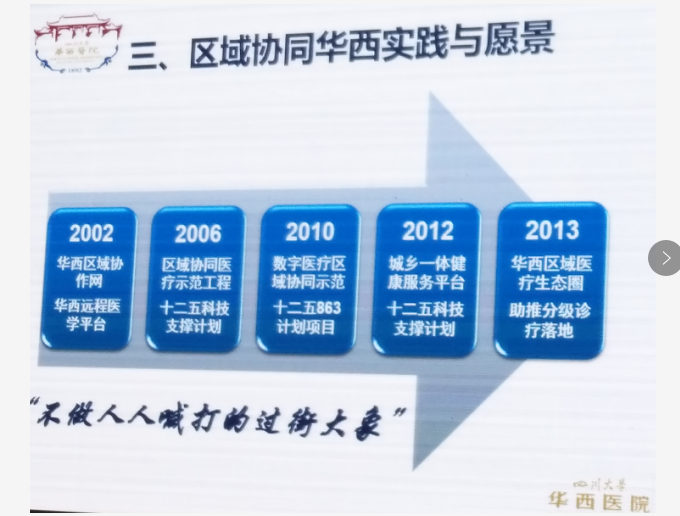
Due to the limited medical resources at West China Hospital, its development model integrates online and offline services, leveraging information technology as a medium.
Overall, after determining the construction model and content, West China Hospital established two types of medical alliances: one is loose-knit, and the other is tightly integrated.
A representative example of the loose-knit model is the West China Remote Network Alliance Hospital. The tight-knit model adheres to the principles of “three unchanged, three shared, and three unified,” and is structured into group-based institutional alliances, led regional alliances, regional specialty alliances, and urban community alliances.
The West China Hospital Loosely Coupled Telemedicine Network, initiated in 2003, currently comprises 633 alliance hospitals distributed across China. The Telemedicine Center serves as a National Medical Education Center and is a Regional Pathology Diagnostic Center accredited by the National Health and Family Planning Commission. Each year, it provides training to over 500,000 individuals and conducts consultations on more than 4,000 complex cases. Notably, the West China Hospital Telemedicine System played a significant role during the Wenchuan Earthquake.
Building on the foundation of West China Hospital’s telemedicine system, in 2009, the National High-Tech Research and Development Program (863 Program) provided further support to West China Hospital. “We began developing the West China Internet-based Collaborative Healthcare Platform. The previous West China telemedicine system was a closed system, where all hospitals could only establish connections with West China Hospital as the central hub. However, the internet-based collaborative platform we invested in after 2009 is an open platform. On this platform, regional central hospitals can establish their own original centers to conduct remote teaching and remote consultations,” said Huang Yong.
Today, this platform has become the foundational infrastructure for the West China Medical Consortium and serves as the key support system for West China Hospital’s institutional services. It primarily facilitates inter-institutional collaborative services, including medical education, remote pathological consultation, imaging diagnosis, remote joint outpatient clinics, and joint ward rounds. By promoting information sharing and symbiotic development, the platform aims to transcend the traditional hospital-to-hospital model, enabling direct ward-to-ward, doctor-to-doctor, and desktop-to-desktop interactions.
Referral services were also implemented. Taking West China Hospital as an example, from the perspective of upward referrals from primary care institutions, the hospital’s beds are fully occupied every day. How, then, can it accept downward-referral patients? Many institutions have called for the establishment of “green channels” (expedited referral pathways), but even when such agreements are signed, they often cannot be effectively implemented. “It is feasible for us to open a green channel to one institution, but if we do so for dozens of institutions, can it still be considered a ‘green channel’? Therefore, managing referrals and acceptances is very challenging,” explained Huang Yong.
West China Hospital’s current approach to managing upwardly referred patients involves joint ward rounds and collaborative diagnosis during the transfer and acceptance process. If a physician determines that a patient should be transferred, they document their recommendation in the system and issue a transfer request form. Such transfers are given top priority; as soon as a bed becomes available, the patient is immediately assigned to it, and both the patient and the receiving hospital are notified, allowing the patient to be admitted directly to the ward.
“This is what we truly mean by a ‘green channel’: negotiations are conducted by physicians, and the authority to allocate resources is vested in them. This ensures that the most valuable resources are directed to the patients who need them most,” said Huang Yong with confidence.
For patients transferred to lower-tier hospitals, the process remains the same. For instance, when a cancer patient needs to be transferred after completing the first cycle of chemotherapy, it is essential to instill confidence in the patient and foster trust in the receiving hospital. This can be achieved through continuous follow-up via joint ward rounds.
For individual services, West China Hospital also offers features such as streamlined medical administrative management, online outpatient consultations, follow-up and rehabilitation for chronic diseases, and chronic disease management. On the physician side, West China Hospital provides mobile applications tailored for both patients and doctors to help physicians manage clinical affairs, specifically by assisting with clinical task management. Huang Yong stated, “It is normal for clinicians to forget things given their heavy workloads; it would be abnormal if they did not. We provide this auxiliary service for task management.”
In the development of led regional medical consortia, West China Hospital primarily enters into agreements with regional governments to deepen cooperative healthcare management. With the government as the principal party to the agreement, West China Hospital takes the lead in managing the regional central hospital, thereby radiating influence and driving the development of county-level hospitals and township health centers, ultimately establishing a tiered and collaborative service system between the entire region and West China Hospital.
So, how exactly does West China Hospital provide leadership? There are two approaches: one is on-site, and the other is online.The affiliated hospitals share the West China Hospital brand, and a management team is assigned, consisting of an Assistant Dean responsible for clinical services and an Operations Assistant responsible for hospital operations. Team members are required to work at the partner hospitals for two days per month and provide on-site support for one month each year. Meanwhile, department chairs must coordinate relevant resources within their departments to deliver both on-site and remote assistance.
In addition to facilitating advanced training for medical staff at hospitals within the medical consortium, West China Hospital also offers short-term training programs. For instance, a team from Jiuzhaigou People’s Hospital came to West China Hospital specifically to learn laparoscopic techniques. After two months, the team returned and was able to implement the corresponding laparoscopic procedures and provide related management consulting services.
Online services, facilitated by the universal health card, enable bidirectional appointment scheduling, sharing of clinical information, online imaging and pathology diagnostics, virtual joint consultations, interdepartmental joint rounds, bidirectional patient referrals, and online educational courses.
West China Hospital has consistently strived to decentralize high-quality medical resources, enhance management quality, improve technical capabilities and service standards, facilitate continuous knowledge transfer, and streamline patient referrals. This approach not only helps hospitals within the medical consortium ensure and improve diagnostic and therapeutic outcomes but also promotes ongoing knowledge dissemination. By establishing a routine operational mechanism, specialist physicians at primary care hospitals can engage in weekly case discussions with West China Hospital physicians, thereby serving as a talent development framework. In this context, the key role for West China Hospital is to sustain continuous knowledge transfer.
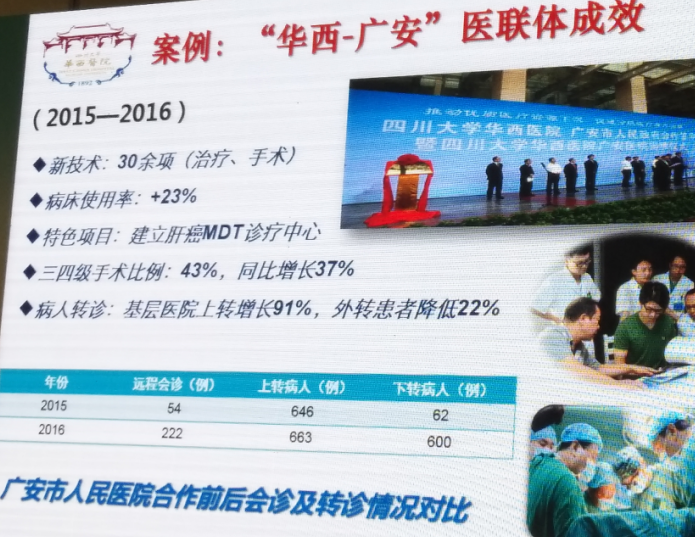
After more than a year of collaboration between West China Hospital and Guang’an primary-care hospitals, the proportion of patients referred upward from the latter increased by 91%, while the proportion of patients transferred outside decreased by 22%.
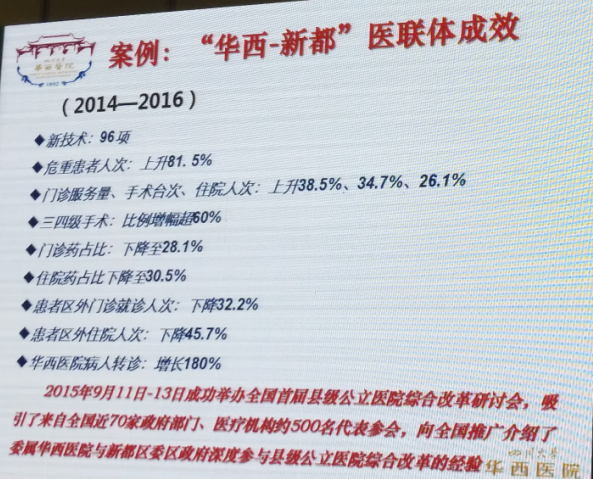
According to data obtained from the Sichuan Provincial Social Security Bureau, after West China Hospital and Xindu District established a medical consortium, the number of patients seeking inpatient care outside the district decreased by 45.7%, and the number of outpatient visits outside the district decreased by 32.2%.
West China Hospital and Ganzi Established a Medical Consortium, Solving the Local Treatment Challenge of Echinococcosis.At the same time, it attracted all 18 county hospitals and 84 township health centers in the region to join the medical consortium platform, forming a complete four-tier hierarchical collaborative service system.
During the development of West China Hospital’s specialty alliances, the primary focus has been on establishing regional specialty alliances. The core components include academic conferences, talent development, collaborative diagnosis and treatment, and two-way patient referrals. These alliances encompass the Hematology Alliance, Cardiology Alliance, Thrombolysis Alliance, and Oncology Alliance. Additionally, there are discipline-specific alliances, including the Laboratory Medicine Alliance, Radiology Alliance, Pathology Alliance, and Nutrition Alliance. In the field of radiology, West China Hospital primarily specializes in CT and MRI services. While primary care institutions possess basic diagnostic capabilities for radiological examinations, cases involving uncertain findings on CT or MRI scans can be referred to West China Hospital for further evaluation.
The core of the West China Urban Community Alliance is to conduct online joint outpatient services. As a general practice base, West China Hospital dispatches general practitioners for regular consultations and specialists for rotating visits, while also facilitating two-way referrals between outpatient and inpatient care.Currently, two-way referral systems have been established with 54 outpatient clinics to serve the community, and services are provided to the community in collaboration with 33 ambulatory surgery centers.

It can be said that this is a pilot area for chronic disease management at West China Hospital. Such an initiative cannot be implemented without patient participation; it cannot be carried out by West China Hospital alone, nor by community health centers alone. A collaborative approach is essential.
Meanwhile, West China Hospital is also establishing its own physician group. With the approval of West China Hospital of Sichuan University, Sichuan Huaxi Hospital Asset Management Co., Ltd.—a wholly-owned subsidiary invested and established by West China Hospital of Sichuan University—has set up the “West China Physician Group.” This group recruits a cohort of clinical physicians who, after undergoing unified training, are dispatched to various locations including the main campus of West China Hospital of Sichuan University, its branch hospitals, and affiliated (cooperative) hospitals to practice as physicians. This initiative facilitates coordinated efforts in hospital management, healthcare services, talent development, and two-way patient referrals.
In addition, West China Hospital will establish the West China Medical Group in accordance with the “Three Unifications” principle, which includes unified internal management, unified administrative departments, and unified resource allocation. The hospitals comprising this group are all affiliated with the West China consortium, including Sichuan Provincial Fifth People’s Hospital and Chengdu Shangjin Nanfu Hospital, among others. Located in the Tianfu New Area, the medical group is building a new tertiary hospital with a capacity of 1,500 beds. Both the management and clinical teams are organized by West China Hospital.
These medical institutions are referred to by Huang Yong as the most tightly integrated healthcare group, truly achieving “three unifications,” and will serve as the vehicle for responding to social insurance global budget prepayment and medical consortiums in the future.
West China Hospital’s medical consortium is not merely a partnership between collaborating institutions, nor is it driven by the goal of mutual benefit; rather, as both a provider and a recipient of healthcare services, it must take societal needs into account.
In Huang Yong’s view, first, tertiary hospitals play a crucial role in establishing medical consortia to implement tiered diagnosis and treatment. Throughout this process, the positioning of tertiary hospitals is vital. Among hospitals at all levels, especially for administrators, it is essential to clearly define the functional role of their institutions. They must have a clear understanding of their own positioning; for instance, West China Hospital also needs to clarify its role by determining which patients to accept and which not to. For example, in the future, West China Hospital may no longer treat common conditions such as the common cold. In fact, within the construction of a tiered diagnosis and treatment system, ensuring the practical implementation of technical capabilities requires a willingness to make concessions on interests, with a greater emphasis on yielding benefits.
A few years ago, West China Hospital found it difficult to meet expectations while assisting grassroots medical institutions, as some of these institutions had boundless demands. For instance, a county-level hospital sought West China Hospital’s help in cultivating a professional team for diagnostic and therapeutic services that it intended to launch despite having no foundational capabilities in those areas.
“Every time we encounter such issues, Huang Yong gets a headache. ‘If all primary care institutions within the medical consortium make such requests, we won’t be able to handle the workload.’”
Second, based on its own positioning, it is necessary to meet more severe challenges. For example, West China Hospital is positioned to focus on the diagnosis and treatment of difficult, critical, and severe diseases. Therefore, it needs to continuously innovate to improve the level of diagnosis and treatment for difficult and critical illnesses, complex diseases, and rare diseases.
Looking ahead, Huang Yong also hopes to receive more suggestions from industry peers on the development of medical consortia and regional collaboration, so as to better implement tiered diagnosis and treatment.
Judging from the current composition of medical consortia led by tertiary Grade A hospitals, there is more interaction between tertiary Grade A hospitals and secondary hospitals, including those at the Grade II Class A or even Tertiary Grade B levels. Does the establishment of such medical consortia truly achieve tiered diagnosis and treatment? Will they remain the mainstay in the future?
Han Guangshu, President of Nanjing Drum Tower Hospital, believes that these medical consortium hospitals should not become the main body of future medical consortia. Similarly, tertiary Grade A hospitals like West China Hospital should not engage in forming medical consortia and should instead step outside the framework of such consortia.
As the medical hub of the entire Southwest region, West China Hospital cannot fully realize its potential if confined within a single medical consortium. Therefore, it should transcend the operational scope of such consortia and assume a guiding role in their development, taking on greater responsibilities to address complex medical challenges that individual hospitals are unable to resolve.
In Han Guangshu’s view, the path toward achieving tiered diagnosis and treatment may require greater policy intervention, such as the design and implementation of patient flow management, with emergencies excluded.
For example, Patient A has a cold. His home is 100 meters away from West China Hospital and 500 meters away from the community health center. Before the implementation of tiered diagnosis and treatment, he would definitely go to West China Hospital for his cold. After the introduction of tiered diagnosis and treatment, restrictions are imposed through the design and enforcement of medical consultation protocols; if patients do not visit the community health center first, they are required to pay higher medical fees.
Perhaps in the process of implementing tiered diagnosis and treatment, various medical institutions such as tertiary hospitals, county-level hospitals, and community health centers will encounter all kinds of difficulties and obstacles. However, there are always more solutions than problems, and we believe that the “inverted triangle” model will eventually be broken.