Building Medical Consortiums: A Clear Guide to the Four Models Promoted by China's Healthcare Reform
“Let resources and technology ‘do more running’ so that patients do less, and guide orderly medical care—this is the original intent behind the government’s vigorous promotion of medical consortia.”
Medical consortia have long been held in high esteem, emerging as the darlings of healthcare reform initiatives across various regions. A diverse array of such consortia has sprung up like bamboo shoots after a spring rain, with the aim of breaking the deadlock in healthcare reform development.
The formal elevation of medical consortium development to a national-level policy occurred on March 5, 2017, when Premier Li Keqiang of the State Council stated in his Government Work Report, “Comprehensively launch pilot programs for the development of medical consortia in various forms, with all tertiary public hospitals participating and playing a leading role.”
Over a month later, Premier Li Keqiang deployed the promotion of medical consortium construction at the State Council’s executive meeting. He pointed out the need to break down barriers in administrative divisions, fiscal investment, health insurance payment, and personnel management, to explore the construction of medical consortia according to local conditions, and proposed four models of medical consortia: urban medical consortia, county-level medical communities, specialized medical consortia, and remote medical collaboration.
So, what are the components of these four types of medical consortiums? Which regions have already demonstrated exemplary benefits? What are their operational processes? What are their respective advantages? And what are some notable best-practice case studies?
In accordance with the “Guiding Opinions of the General Office of the State Council on Promoting the Construction and Development of Medical Consortia,” all localities shall, based on the actual status of their tiered diagnosis and treatment system development, adopt measures tailored to local conditions and provide categorized guidance. They shall fully consider factors such as the geographic distribution, functional orientation, service capacity, operational relationships, and willingness to cooperate of medical institutions, leverage the roles of various medical resources from central and local governments, the military, and society, respect grassroots innovation, and explore the formation of diverse models of medical consortia by region and hierarchy. This aims to facilitate the flow of high-quality medical resources to primary care settings and remote, impoverished areas. Private medical institutions may be incorporated into medical consortia based on their willingness.
It can be seen that both public and non-public medical institutions may participate in medical consortiums, with participation by non-public medical institutions being voluntary.
Between urban and rural areas, with tertiary public hospitals in cities as the main entities, medical consortia are established through various forms such as trusteeship of county-level hospitals within the region, building on already established long-term and stable counterpart support relationships. Tertiary public hospitals can dispatch management teams and expert teams to county-level hospitals, focusing on assisting and enhancing the medical service capabilities and standards of these county-level hospitals.
National- and provincial-level public hospitals, in addition to participating in local medical alliances, may establish cross-regional cooperative relationships with multiple medical alliances to form high-level, complementary medical alliances. These alliances should carry out innovative collaborative research, promote the widespread adoption of technologies, and cultivate talent, thereby radiating influence and driving the enhancement of regional medical service capabilities.
So, what exactly are the workflows of these four types of medical consortia?
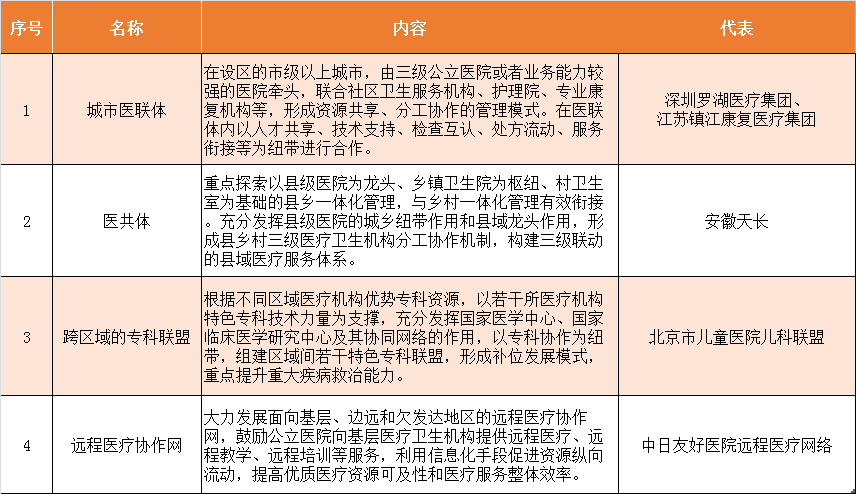
1、Urban Medical Consortium (i.e., Medical Alliance), divided into tightly-knit and loosely-knit types,Led by a tertiary hospital, in collaboration with several urban secondary hospitals, rehabilitation hospitals, nursing homes, and community health service centers, to establish a “1+X” medical consortium, vertically integrating healthcare resources to form a management model characterized by resource sharing and division of labor.
Flowchart for Two-Way Referral in the Regional Medical Consortium of The Second Affiliated Hospital of Guangzhou Medical University (abbreviated as “GMUH Second Hospital”):
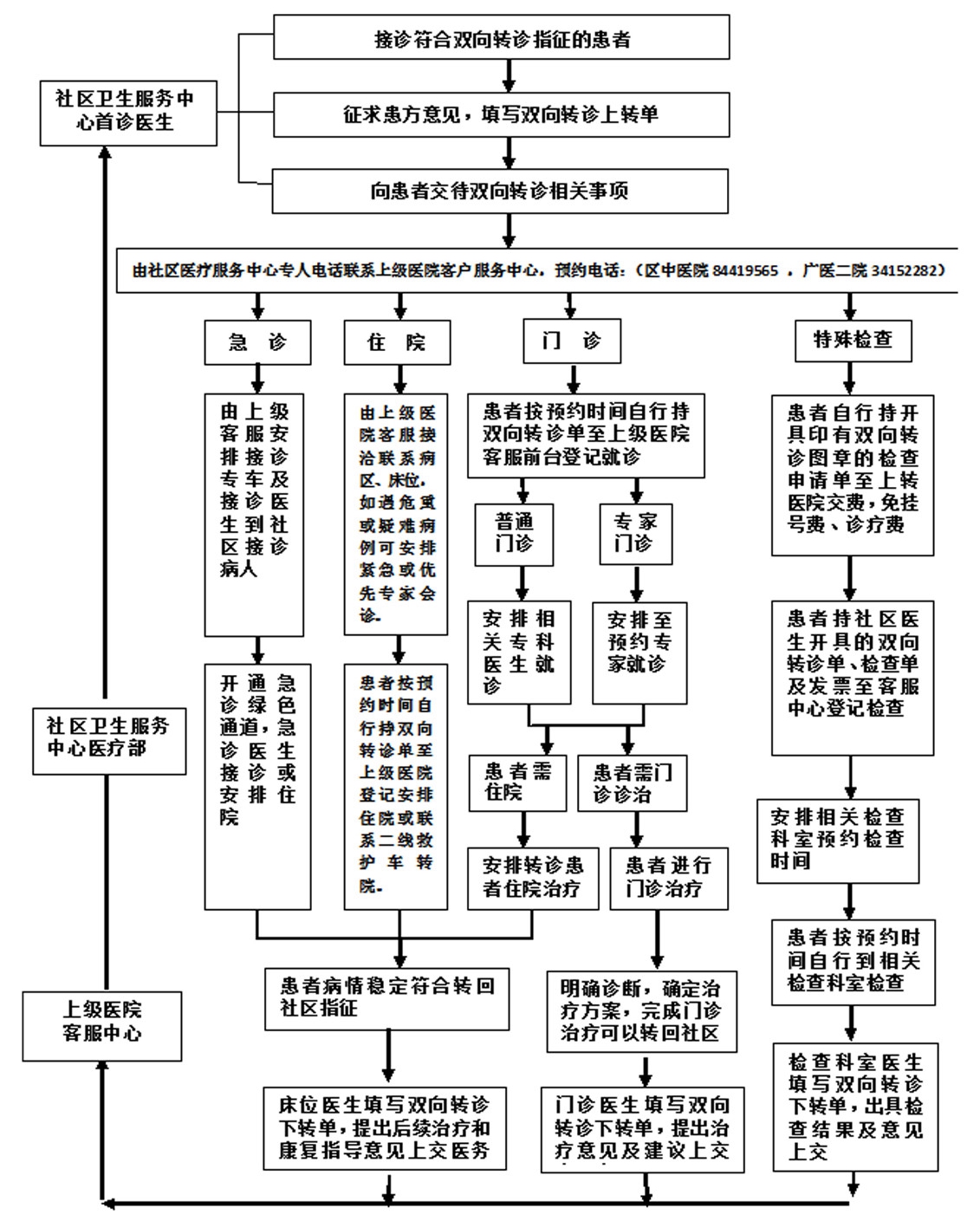
As can be seen from the list, the Second Affiliated Hospital of Guangzhou Medical University is a typical representative of a close-knit urban medical consortium. It features three characteristics:
First, community health centers and tertiary hospitals have achieved integrated management of personnel, finances, and materials. Structurally, this forms a regional, vertically integrated, tightly coupled medical consortium linked by property rights, thereby balancing both economic interests and technical collaboration.
Second, the medical technology systems, nursing quality, sterilization supply, logistics maintenance, and equipment procurement have been brought under the unified management of Grade A tertiary hospitals;
Third, community health centers are better equipped to fulfill public health and primary care mandates assigned by the government. Characteristic services such as “grid-based service delivery” and “family doctor programs” have been consolidated and expanded, fostering a regional healthcare service system with tertiary hospitals that features “vertical integration, division of labor and collaboration, and combined prevention and treatment.”
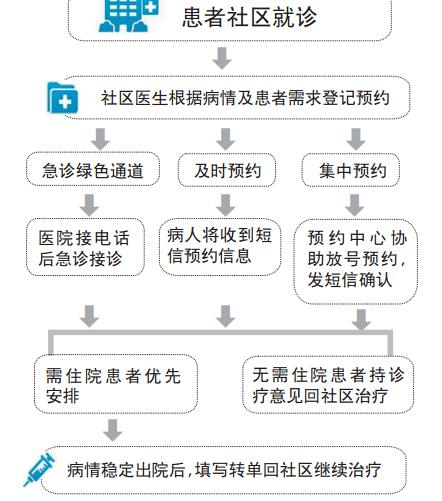
2. Medical Community (i.e., Healthcare Consortium),This is the primary model for developing medical consortiums in rural areas. By closely integrating health insurance payment reform with the construction of medical communities, it provides integrated services spanning prevention, treatment, and rehabilitation, thereby linking county, township, and village levels.
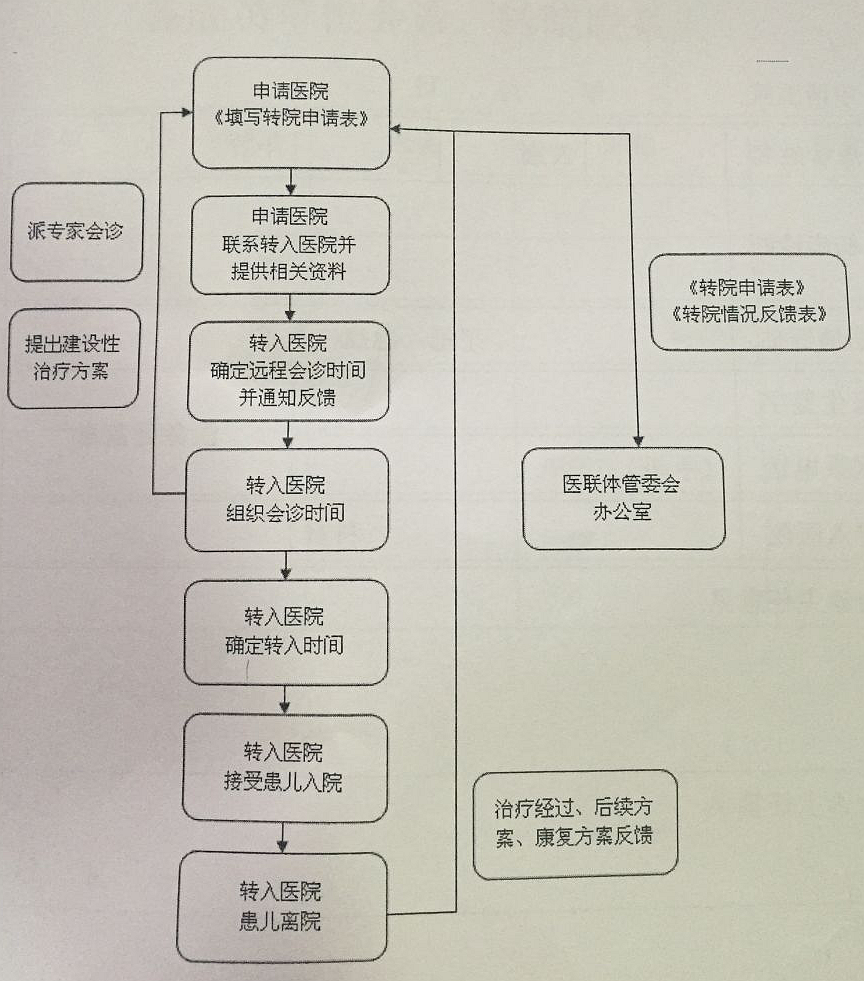
3. Cross-Regional Specialty AlliancesA medical consortium is a collaborative alliance formed among healthcare institutions, linked by specialty cooperation. Centered on the distinctive specialties of one leading institution, it integrates specialized expertise from other institutions to establish several regional centers of excellence. This model enhances the capacity to manage and treat major specialty-specific diseases and fosters a complementary development pattern. For example, the patient transfer process within the Anhui Provincial Pediatric Medical Consortium:
4. Telemedicine Collaboration NetworkThis involves the establishment of a telemedicine service network by leading institutions in collaboration with medical facilities at the primary care level and in remote, underdeveloped regions. By leveraging information technology, this approach promotes the vertical flow of medical resources, enhances the accessibility of high-quality medical resources, and improves the overall efficiency of healthcare services.

It can be seen that there are four applicable scenarios for telemedicine collaboration networks:
One is hospitals, facilitating remote consultations among experts;
One is schools and research institutions;
One is emergency first aid;
One is family guardianship.
Meanwhile, telemedicine within the medical consortium enables seamless connectivity from primary care hospitals to large tertiary hospitals, significantly facilitating local patients in receiving effective treatment without leaving their county.
As the new healthcare reform advances, although the medical consortium model features clear processes, it also faces severe challenges.
From the perspective of urban medical consortia, a “1+X” collaborative operational model is established with tertiary Grade A hospitals as the lead institutions. This places higher demands on the financial and technical support capabilities of the lead hospitals, necessitating more robust performance evaluation and compensation mechanisms for physicians from tertiary Grade A hospitals who provide assistance to primary healthcare institutions.
For loose-knit medical consortia, tertiary Grade A hospitals and their member institutions are not truly “one family.” On the one hand, conflicts of interest exist among members. Public hospitals operate under a mechanism where they retain their own revenue and distribute surpluses; therefore, implementing consortium initiatives—such as dispatching medical staff—increases costs, while diverting patients reduces income. On the other hand, objective constraints make implementation difficult. For example, incompatible information systems prevent the interoperability and sharing of diagnostic and treatment data; inconsistent standards for medical quality and test results lead to non-recognition of diagnostic outcomes across institutions; high costs and low efficiency hinder physician mobility and communication, reducing the incentive for large hospitals to help smaller ones improve their technical capabilities; medical resources struggle to flow downward to primary care levels, resulting in a situation where upward referrals of patients are easy, but downward referrals are difficult.
Therefore, even with the expansion of medical consortiums, large hospitals remain the primary beneficiaries; small hospitals continue to experience stagnation in medical service quality and struggle to retain patients.
If medical institutions can form tightly integrated medical consortia, the member units within the system will achieve unified allocation and management of human resources, finances, and materials, as well as integration of economic interests, thereby resolving the most significant conflict-of-interest challenges facing the development of such consortia.
Aligning the interests of large tertiary hospitals with those of primary care institutions serves a dual purpose: on one hand, tertiary hospitals assist smaller facilities in enhancing their medical expertise and service quality, thereby reversing the current trend of low patient volume; on the other hand, this collaboration alleviates overcrowding and reduces excessive wait times for registration, consultation, and medication while shortening actual consultation duration at tertiary hospitals. This allows them to focus more on tackling complex and refractory diseases and advancing medical standards, thus fully leveraging their leading role in the healthcare system.
The challenge in building specialized medical consortia lies in their reliance on disciplinary support from tertiary Grade A hospitals, as primary healthcare institutions indeed have limited expertise in managing specific diseases, which undermines the sustainability of two-way referrals within these specialized alliances. Although targeted disciplinary assistance helps improve the specialized diagnostic and treatment capabilities of primary care facilities, the training cycle required is excessively long.
Another set of challenges associated with remote collaboration networks is even more pronounced: currently, they can only address the consultation component of medical history taking, while many auxiliary examination records are not immediately accessible; medical insurance does not yet cover the costs of remote consultations; there is no clear mechanism for accountability in cases of misdiagnosis or missed diagnosis; and there is a lack of face-to-face care during the medical consultation process.
Although medical consortiums face numerous challenges, there are still successful cases. For example, the urban medical consortium—Luohu Hospital Group; and the medical community—Tianchang, Anhui.
First, the medical consortium of Shenzhen Luohu Hospital Group is a tightly integrated medical alliance. In August 2015, Luohu District consolidated five district-level public hospitals and 35 community health centers into a single legal entity, established a corporate governance structure, and founded the Luohu Hospital Group. Following the reform, healthcare resources within the district were comprehensively integrated and optimized, with the establishment of six resource-sharing centers and six administrative management centers to reduce operational costs. Notably, the medical group facilitates talent sharing, technical support, mutual recognition of examination results, prescription portability, and seamless service coordination among its member institutions.
According to Sun Xizhuo, President of Luohu Hospital, “Luohu Hospital has integrated resources and established a hospital group not to attract more patients, but to strengthen community health centers, improve residents’ health levels, and reduce the overall number of people with diseases.”
Luohu Hospital has also made experience in community health centers a criterion for the professional title and job promotion of medical staff, and strengthened fiscal policy guidance by providing subsidies for experts to deliver lectures, conduct free clinics, hold outpatient sessions at non-community health center-affiliated facilities, and provide weekend outpatient services at community health centers, thereby making such deployments an integral part of their duties. These experts are required to be assigned to community health centers to provide residents with medical care, prevention, healthcare, mental illness prevention and control, and chronic disease management services.
Therefore, in 2016, the outpatient volume at the community health centers under the direct administration of the Luohu Hospital Group increased by 94.6% year-on-year, and the proportion of basic medical insurance enrollees within the jurisdiction seeking care at the Group’s community health centers rose from 51.47% to 60.3%.
Next is the “Tianchang, Anhui” Medical Consortium. The aim is to promote vertical integration of medical resources, improve the urban-rural medical service system, and simultaneously enhance the medical service capabilities at both the county and township levels.
According to Yang Furen, Director of the Tianchang Municipal Health and Family Planning Commission, prior to the implementation of the “Medical Community,” healthcare utilization in Tianchang was characterized by a pronounced polarization: county-level hospitals were overcrowded, while township health centers saw very few patients. To address this disparity and establish a smooth tiered diagnosis and treatment system within the county, Tianchang embarked on healthcare reform initiatives centered on the development of “Medical Communities.”
Specifically, the “Medical Consortium” comprises four dimensions: a service community, an interest community, a responsibility community, and a development community. These four aspects are interrelated and mutually influential.
For instance, the “Service Community” integrates medical services at the county, township, and village levels, leveraging their respective strengths to achieve coordinated prevention, treatment, and rehabilitation. Meanwhile, the “Responsibility Community” clearly defines the scope of practice for county-level public hospitals and township health centers, such as ensuring a catalog of diseases treated at these two tiers, along with lists of 41 disease types and 15 conditions in the rehabilitation phase designated for downward referral from county-level hospitals.
Among the conditions included in the mandated admission list, county-level hospitals cover 122 diseases, while township health centers cover 50. Patients with these listed conditions must not be arbitrarily transferred to higher-level facilities; otherwise, they will forfeit preferential medical insurance reimbursement policies. For instance, stroke patients can be transferred down to township health centers. After passing the critical phase, such patients typically require prolonged rehabilitation, at which point they should be transferred to township hospitals. Continuing rehabilitation at county-level hospitals would result in long-term bed occupancy and higher costs, whereas township hospitals are fully capable of providing the necessary rehabilitative care for these conditions.
In this way, stroke patients avoid long-term bed occupancy at county-level hospitals, address the issue of patient shortages at township health centers, and benefit from higher reimbursement rates, achieving multiple benefits simultaneously.
For specialized medical consortia, targeted specialty assistance helps enhance the diagnostic and treatment capabilities of primary care hospitals; meanwhile, it facilitates the upward referral of complex cases to tertiary hospitals, thereby achieving effective departmental alignment within the consortium.
The specific approach involves selecting a medical institution with strong specialized technical capabilities to take the lead, helping primary healthcare institutions improve their diagnostic and treatment capabilities for specialized diseases, and assisting them in building a “permanent medical team” that cannot be taken away, thereby transforming traditional “assistance” into long-term cooperation. For example, Beijing Children’s Hospital.
According to Ni Xin, President of Beijing Children’s Hospital, the hospital has been as crowded as a railway station during the Spring Festival travel rush since she assumed office in 2012. To better meet the medical needs of pediatric patients and alleviate the severe overcrowding at Beijing Children’s Hospital, Ni Xin launched another initiative in 2013—establishing the Beijing Children’s Hospital Group across provincial boundaries—building upon the Beijing Pediatric Comprehensive Service Platform established in 2012.
By facilitating academic exchanges, establishing research platforms, implementing co-developed departments, providing remote consultations, and deploying expert teams for touring diagnoses and surgeries across various regions, the Beijing Children’s Hospital Group has enhanced the comprehensive capabilities of its member hospitals. This initiative has driven the overall improvement of pediatric care across China, enabling patients to access first-class diagnostic and treatment services without leaving their provinces.
Initially, the Beijing Children’s Hospital Group comprised only nine member institutions; today, it has expanded to include more than 700 members. As the largest cross-provincial medical consortium in China, its membership primarily covers North China, South China, Southwest China, and Central China. By facilitating sharing among member institutions across six domains—expertise, clinical practice, scientific research, teaching, management, and prevention—and by establishing a telemedicine consultation center, the Group aims to achieve the goal of “patients stay put, while experts move.”
VCBeat analyzed outpatient visit data from 2014 to 2015. In 2014, Beijing Children’s Hospital recorded 3.37 million outpatient visits, which decreased by approximately 200,000 in 2015. This indicates that the hospital’s cross-regional specialized medical consortium has achieved preliminary results.
How can we enhance the capacity of primary healthcare services in remote mountainous areas? The practices of China-Japan Friendship Hospital may offer some insights.
It is understood that China-Japan Friendship Hospital was among the early institutions to explore telemedicine. In 2012, with the approval of the former Ministry of Health, the “Ministry of Health Telemedicine Management and Training Center” was established at the hospital, primarily engaged in telemedicine services and the formulation of related policies, regulations, and standards.
Nowadays, telemedicine collaboration networks, represented by the China-Japan Friendship Hospital Telemedicine Network, are service networks established between leading institutions and medical facilities in primary care, remote, and underdeveloped areas. Public hospitals provide services such as remote medical consultations, remote teaching, and remote training to primary care, remote, and underdeveloped regions. These initiatives leverage information technology to facilitate the vertical flow of resources, enhance the accessibility of high-quality medical resources, and improve the overall efficiency of healthcare services. Efforts are being made to address issues such as inconsistent technical standards for telemedicine and barriers to information sharing and interoperability among systems. By further demonstrating the exemplary role of telemedicine, establishing national standards and norms for its development, and promoting sustainable growth through training and dissemination, these initiatives aim to foster the sustainable development of telemedicine in China.
Peng Mingqiang, Vice President of China-Japan Friendship Hospital, stated that with the development of “Internet Plus,” telemedicine services are continuously expanding. According to statistics, China-Japan Friendship Hospital conducted over 5,000 remote consultations in both 2015 and 2016, and this year’s figure is expected to far exceed that level.
Currently, China-Japan Friendship Hospital maintains collaborative partnerships with over 2,000 medical institutions across China. After several years of development, the scope of its telemedicine services has continued to expand, encompassing not only remote consultations but also remote training and education.
Because primary healthcare facilities are relatively underdeveloped, primary care physicians do not encounter many complex or rare cases. Therefore, Peng Mingqiang believes that in terms of infrastructure, telemedicine primarily serves hospitals at the municipal level or above (including county-level hospitals). The quality of corresponding diagnostic imaging, such as CT and MRI scans, is generally adequate; the main limitations lie in differential diagnostic and overall diagnostic capabilities.
Therefore, by conducting regular training sessions focused on the analysis of typical cases and complex or rare conditions, and by leveraging case-based learning to train primary care physicians, we aim to enhance their diagnostic and treatment capabilities.
To excel in telemedicine, it is essential to first shift mindsets, optimize organizational structures, establish dedicated telemedicine centers, and assign specialized personnel for coordination.
Furthermore, standards and procedures must be streamlined. For instance, a standardized protocol must be established for hospital operations upon receiving requests for remote consultations, including the arrangement of specialist participation. The remote medical center should fulfill roles in management, coordination, and service provision, while also mobilizing the enthusiasm of primary care physicians to jointly promote the development of telemedicine in China.
In terms of the distance between patients and hospitals, as medical consortiums have proliferated across the country, the time patients spend traveling for medical care has been decreasing. Liang Wannian, Director of the Department of Structural Reform under the National Health and Family Planning Commission, stated, “In the long run, if the division of labor among medical institutions within a medical consortium is clearly defined, their roles are well-positioned, and assessment and evaluation mechanisms aligned with the consortium model are established, closely-knit medical consortiums will yield better outcomes. Currently, we encourage the development of closely-knit medical consortiums without imposing mandatory requirements, allowing for diverse models.” He added that the most important principle in building medical consortiums is to shift the focus from emphasizing the efficiency of individual medical institutions to enhancing the overall efficiency of the entire healthcare service system.