Yi Yanhua of Kingdee Healthcare: Electronic Medical Records and Health Big Data—Regional Application Is the Future
With the implementation of national policies on health and medical big data, electronic medical records, as one of the foundational databases, are integrated into hospital information systemsChina's status continues to rise. In response toElectronic Health Records in Healthcare Big Datadevelopment issues, VCBeat (WeChat Official Account: vcbeat) conducted an exclusive interview withExperts from several of the most representative electronic medical record (EMR) companies in China.
As a pioneer in domestic hospital management models and mobile internet hospitals, Kingdee Medical has currently provided informatization services to over 3,000 hospitals and healthcare institutions.
Its business portfolio covers Digital Hospitals (H-ERP, HIS, LIS, EMR & CP), Mobile Internet Hospitals (Patient Mobile Service Platform, Mobile Work Platform, Mobile Supply Chain E-commerce Platform), and Cloud Hospitals (Cloud HIS, Online Consultation and Telemedicine Platform, Medical Consortium and Tiered Diagnosis and Treatment Platform).
As of June 22, 2017, Kingdee Medical’s mobile internet hospital platform had served over 11.26 million users and facilitated more than 19.78 million direct hospital payment transactions, ranking among the leading providers in China.
In exploring the application of big data in healthcare, Kingdee Healthcare aims to build a big data-based health management and service platform to provide patients with wellness, rehabilitation, and healthcare services. By matching symptoms, the platform facilitates tiered diagnosis and treatment. Leveraging big data, it tracks the closed-loop medication process to empower personalized research and development.
To gain insight into Kingdee Healthcare’s progress in electronic medical records (EMR) and healthcare big data, VCBeat conducted an exclusive interview withYi Yanhua, Dean of the Kingdee Medical Innovation Research Institute。

![]() Dr. Yi Yanhua serves as the Dean of the Innovation Research Institute at Kingdee Medical Software Technology Co., Ltd. He holds a Ph.D. in Preventive Medicine from Prince of Songkla University (Thailand), a Master’s degree in Urology from Guangxi Medical University, and dual bachelor’s degrees in Clinical Medicine and English from University of South China. His primary research interests include clinical epidemiology, medical education, health human resources, and data analysis and mining.
Dr. Yi Yanhua serves as the Dean of the Innovation Research Institute at Kingdee Medical Software Technology Co., Ltd. He holds a Ph.D. in Preventive Medicine from Prince of Songkla University (Thailand), a Master’s degree in Urology from Guangxi Medical University, and dual bachelor’s degrees in Clinical Medicine and English from University of South China. His primary research interests include clinical epidemiology, medical education, health human resources, and data analysis and mining.
Dr. Yi Yanhua was one of the three Chinese recipients of the 2012 China Medical Board (CMB) Fellowship. In the past year, he has published eight papers indexed by SCI/EM. He studied under Professor Virasakdi Chongsuvivatwong, a world-renowned epidemiologist and statistician and the creator of the R packages EpiDisplay and EpiCalc, and has conducted in-depth research on the application of software in the analysis of clinical medical research data.
Digitization, Structuring, Standardization, and Regionalization: The Four Stages of Electronic Medical Record Development
Healthcare big data is primarily categorized into three major components: pre-hospital data, in-hospital data, and post-hospital data.
Pre-hospital data includes patients’ diagnostic and treatment activities, lifestyle habits, and other factors. These data are collected via mobile devices. Post-discharge data are primarily collected by the post-diagnosis management system. Electronic medical records (EMRs) undoubtedly belong to in-hospital data, representing the core component of clinical diagnostic and treatment data.
The industry generally divides the development of electronic medical records into four stages:
The first phase is the digitization of paper-based medical records.In the past, paper-based medical records had to be filled out manually by physicians; if there were three or more alterations, the entire record had to be rewritten, which was both time-consuming and labor-intensive. The digitization of data involves storing originally handwritten information in electronic format. This enables physicians to perform all operations rapidly via computer.
Phase 2 is data structuring.Given the variability in medical records documented by different physicians, standardizing medical record data has become a top priority. The emergence of structured electronic medical records (EMRs) effectively addresses this issue. This approach not only facilitates the extraction of specific data fields for scientific analysis but also standardizes physicians’ documentation practices, thereby enhancing the ease of future retrieval and review.
The third phase is data standardization.With the advancement of hospital informatization, there is a growing need for information sharing and mutual utilization among various departmental systems. The prerequisite for achieving data sharing and interoperability is that data exchange between these systems must adhere to standardized specifications. In this regard, the Chinese government has successively issued guiding documents such as the "Basic Architecture and Data Standards for Electronic Medical Records" and the "Specifications for Shared Documents of Electronic Medical Records." Many hospital information systems have participated in the Interconnectivity Maturity Assessment, laying the foundation for future data applications.
The fourth stage is data regionalization.In the past, electronic medical record (EMR) systems varied across different hospitals. The development of big data in healthcare and cloud technology has enabled individual hospitals to break free from data silos. Regional data integration has become the core focus at this stage. Hospitals not only need to achieve interconnectivity but also establish comprehensive, lifecycle-oriented health big data for patients. In this way, clinical data generated by patients across different hospitals can be seamlessly integrated.
Structured Electronic Medical Records: The Foundation of Health and Medical Big Data
During scientific research, hospitals need to classify data by fields. Data such as gender, age, and disease diagnosis can be structured.
In medical records, such information is highly fragmented, and documentation styles vary among physicians. Therefore, rapidly converting textual data into structured data would facilitate clinical research and analysis.
Structured electronic medical records not only standardize clinical practice but also facilitate scientific research analysis and in-depth data mining by physicians.
To use an analogy, structured electronic medical records (EMRs) divide EMR data into numerous small compartments, each labeled according to physicians’ varying areas of interest. This allows physicians to quickly locate specific compartments via these labels when needed.
Kingdee Medical’s electronic medical record (EMR) system utilizes a proprietary EMR editor with independent intellectual property rights. Currently, its primary market is in South China, where more than 100 hospitals have adopted Kingdee Medical’s EMR system.
Regional Application of Electronic Medical Records
Kingdee Medical’s Regional Electronic Medical Record (EMR) Repository utilizes middleware technology to connect the regional EMR platform with Hospital Information Systems (HIS) across various hospitals for data acquisition, transmitting the data to a regional data center to achieve interoperability among healthcare institutions.
Although technically feasible for quite some time, regional sharing of clinical data in hospitals remains underdeveloped due to limitations in policy openness and the extent of hospital implementation.
In 2015, Kingdee Healthcare achieved data interoperability among five hospitals: Foshan First People’s Hospital, Foshan Traditional Chinese Medicine Hospital, Foshan Maternal and Child Health Care Hospital, Foshan Fifth People’s Hospital, and Gaoming District People’s Hospital.
At these hospitals, Kingdee Medical has established standards for the unified exchange of heterogeneous systems across different institutions, implemented standardized coding for electronic medical records (EMRs), and achieved cross-institutional data integration. In simple terms, patients from any of the five hospitals can be identified and have their data archived at any other hospital, thereby eliminating data silos.
Kingdee Cloud Hospital: Enabling Regional Data Sharing
Kingdee Cloud Hospital is the third-generation hospital information system, newly developed based on Kingdee Medical’s first two generations of products: the Digital Hospital and the Mobile Internet Hospital. Guided by the core principles of openness and sharing in cloud computing, it enables online-to-offline service models through a “cloud + terminal” architecture and achieves refined hospital management via end-to-end closed-loop processes, thereby helping hospitals transform and upgrade their service and management models in the cloud era.
Cloud hospitals break away from the traditional siloed construction model of digital hospitals (such as HIS, LIS, and EMR) by adopting a layered cloud computing architecture (IaaS, PaaS, SaaS). This approach categorizes hospital information services into six major business domains and 122 application modules, with the overall architecture illustrated in the figure below:
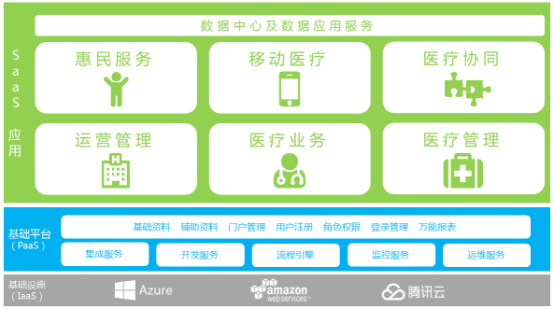
(Kingdee Medical Cloud Hospital Overall Architecture Diagram)
Among these, the medical service management of cloud hospitals is primarily patient-centered and electronic medical record (EMR)-centric, aiming to meet the information needs of clinical diagnosis and treatment, optimize medical processes, improve healthcare quality, ensure patient safety, reduce medical errors, and enhance medical efficiency.
The main modules include outpatient and emergency electronic medical records, outpatient and emergency prescriptions, outpatient infusion services, inpatient electronic medical records, inpatient physician orders, nursing documentation, clinical pathways, clinical laboratory information management, surgical request management, and follow-up service management.
The emergence of cloud hospitals can effectively address the issue of interoperability among information systems, enabling data sharing and exchange. Meanwhile, it facilitates the integration of hospital systems with external platforms, achieving regional data sharing and laying the foundation for application development.
Furthermore, Kingdee Healthcare has conducted joint research with the National University of Singapore to provide scientific research and analytical support services to healthcare institutions within the region. This collaboration has facilitated the analysis of patient healthcare-seeking behaviors, yielding research findings on clinical and care-delivery aspects, such as the impact of insurance systems on patients’ decisions regarding cesarean sections. Moving forward, Kingdee Healthcare plans to develop regional, personalized, proactive health services based on electronic medical record (EMR) data.
The value of data depends on the user and application scenario.
Hospital basic data can be divided into three categories:
1. Clinical baseline data.Including diseases, clinical pathways, medication, etc.
2. Hospital resource data.Including resource data on personnel, finances, and materials, such as cost of sales and treatment expenses.
3. Pre-hospital and post-discharge patient data.including relatively fragmented data such as user behavior, dietary intake, and physical activity.
From the perspective of Kingdee Medical, clinical baseline data in hospitals are supported by systems such as HIS, LIS, and EMR. For hospital resource data, Kingdee Medical utilizes the HRP system for management. Meanwhile, patient behavior data can be collected through various mobile terminals or data acquisition devices.
For instance, physicians need to monitor the amount of social resources consumed by a specific disease and determine the reimbursement rate that the national insurance payment system should cover, which involves data from the Hospital Resource Planning (HRP) system.
By leveraging interoperable information systems to acquire clinical and financial data related to specific disease types, conducting precise cost calculations for these diseases based on clinical pathways, and then comparing hospital disease-specific costs with medical insurance payment standards, the reimbursement rate for the diseases can be determined.
If physicians focus on clinical diagnosis and treatment practices and aim to improve therapeutic outcomes and clinical efficacy in diabetes management, they should place greater emphasis on data related to disease diagnosis, treatment, medications, and post-consultation follow-up.
This requires support from systems such as Electronic Medical Records (EMR). By leveraging disease-specific cost analysis, hospitals can optimize departmental services, provide quantitative recommendations for departmental development, and establish reference indicators for disease-based performance management.
From the perspective of target users, the application of health and medical big data mainly encompasses three aspects:
First, to serve physicians.Enhance their clinical diagnostic and treatment practices, and optimize clinical decision-making.
Second, it serves hospital administrators.Assist them in conducting cost accounting to support government decision-making.
Third, serving patients.By establishing health models and integrating patient genomic data, hospitals can develop disease prediction models and intervention strategies for various conditions, thereby providing patients with guidance on healthy behaviors.
In summary, the data collected by Health IT (HIT) enterprises and the research conducted by medical researchers vary across different application scenarios. The value of data depends not only on its users but also on the specific application context.
Series on Electronic Medical Records and Healthcare Big Data: