Five Key Dimensions of Electronic Medical Records: Standardization as the Foundation for AI and Healthcare Big Data Implementation
Electronic Medical Records: The Foundational Database for Health and Medical Big Data
As is well known, an Electronic Medical Record (EMR) is a data integration system created, stored, and used in electronic form by healthcare institutions, focusing on clinical diagnosis, treatment, and guided intervention information for outpatients, inpatients (or health management subjects). It constitutes a complete and detailed resource of clinical information generated and recorded during an individual’s successive visits to healthcare institutions.
It includes the medical record face sheet, progress notes, examination and test results, physician orders, operative records, nursing records, and more. It contains both structured data and unstructured free text, as well as graphical and image information, encompassing processes such as the collection, storage, transmission, quality control, statistical analysis, and utilization of patient information.
Electronic medical records (EMRs) are the digital personal health records of the new era, encompassing nearly all of a patient’s past and present medical information. As EMR systems become increasingly prevalent in healthcare institutions and clinical data continues to accumulate, the concept of big data in healthcare has gradually emerged.
By leveraging vast amounts of medical big data, healthcare professionals can identify critical evidence related to healthcare quality, patient safety, and drug efficacy through data analysis, thereby enhancing the quality and efficiency of public healthcare, strengthening medical safety, and promoting the research and development of new therapies and pharmaceuticals.
The “Guiding Opinions of the General Office of the State Council on Promoting and Regulating the Application and Development of Health and Medical Big Data,” issued by the State Council in 2016, pointed out that various medical and health institutions should be encouraged to advance the collection and storage of health and medical big data, strengthen application support and operational and maintenance technical safeguards, and open up channels for data resource sharing. Accelerate the construction and improvement of foundational databases centered on residents’ electronic health records, electronic medical records, and electronic prescriptions.
It is also evident that electronic medical records, as one of the foundational databases for big data in healthcare, will play a significant role in the future development of the medical industry.
However, as the application of electronic medical records (EMRs) is not yet mature in China, leveraging clinical data from EMRs for big data analytics or scientific research requires addressing a series of standardization issues, including documentation, coding, functionality, interoperability, management, and usage. Only by standardizing and regulating non-standardized scenarios can the data extracted from EMRs be ensured to be authentic, continuous, and complete.
Only in this way can a solid foundation be laid for the interconnectivity among medical institutions, enabling third-party enterprises specializing in informatization, big data, and artificial intelligence to better leverage technology to extract valuable insights from health and medical big data, thereby helping medical institutions improve the health status of residents.
In response, VCBeat has compiled the electronic medical record-related5 Key Standardized Components:
I. Standardization of Electronic Medical Record Documentation
In 2010, the Ministry of Health issued the Basic Standards for Medical Record Documentation (hereinafter referred to as the “Standards”), which clearly defined medical record documentation (including electronic medical records) as the process by which healthcare professionals obtain relevant data through medical activities such as patient interviews, physical examinations, auxiliary tests, diagnosis, treatment, and nursing care, and then summarize, analyze, and organize these data to create records of medical activities.
The Specifications not only establish standards for the content and requirements of outpatient (including emergency) and inpatient medical records, but also repeal the Basic Standards for Medical Record Writing (Trial) (Wei Yi Fa [2002] No. 190) issued in 2002. This writing specification,MeanwhileIt also laid the foundation for structured standards for electronic medical records.
II. Standardization of Terminology and Coding in Electronic Medical Records
In December 2009, the Ministry of Health and the State Administration of Traditional Chinese Medicine jointly promulgated the "Basic Architecture and Data Standards for Electronic Medical Records (Trial)."
"Basic Architecture and Data Standards for Electronic Medical Records (Trial)" is the first national-level basic specification for electronic medical record business architecture and data standards with characteristics of integrating traditional Chinese and Western medicine, formulated and issued in China's health sector. Since its trial implementation, it has played a positive role in promoting the sharing of patients' medical information within regional areas, as well as interconnectivity and collaborative services among medical institutions.
In recent years, to further promote the development of medical services and provide guidance and standards for the advancement of healthcare, the "Basic Architecture and Data Standards for Electronic Medical Records (Trial)" urgently needs to be revised and improved.
Based on this, the Ministry of Health included the standard for the “Basic Data Set for Electronic Medical Records” as one of the key projects in its “2011 Plan for the Development and Revision of Health Standards.”
Led by the Statistical Information Center of the Ministry of Health, this project involved multiple hospitals, including the Chinese People's Liberation Army General Hospital, and prominent domestic medical IT enterprises such as Neusoft Group and DHC Software, in the joint development of standards. An expert working group for the development of the Basic Data Set Standards for Electronic Medical Records was formed by selecting experts from the participating institutions who had long-term experience in clinical practice, health information standardization, hospital management, and information technology. The work on formulating and revising the standards was launched in June 2011.
The key to establishing dataset standards lies in the selection and standardization of data elements, which determine the usability and scientific rigor of the dataset standards. The primary basis for selecting data elements in the new version of the standard is the operational standards and specifications issued by the health industry since 2009.
These primarily include health industry standards such as the “Specifications for Medical Record Documentation (2010),” “Basic Specifications for Electronic Medical Records (2010),” “Basic Specifications for Traditional Chinese Medicine Electronic Medical Records (2010),” “Front Page of Inpatient Medical Records (2011),” and “Front Page of Inpatient Medical Records for Traditional Chinese Medicine (2011).” All data items explicitly required for documentation in the aforementioned standards are considered for inclusion in the corresponding datasets.
However, whether a data item is selected as a data element for inclusion in the basic dataset requires further analysis based on the complexity of its recorded content. Data items with simple and clear content, such as gender, age, and occupation in the patient’s basic information, can be directly included in the basic dataset. In contrast, data items with complex content, such as “history of present illness” and “past medical history,” need to be analyzed from the perspective of clinical knowledge.
The primary basis for the revision of the “Basic Data Set for Electronic Medical Records” is a series of medical practice standards formulated and promulgated by health authorities in recent years, including both the Western medicine-oriented standards issued by the former Ministry of Health and the traditional Chinese medicine (TCM) practice standards issued by the National Administration of Traditional Chinese Medicine. Examples include the “Specifications for Medical Record Writing (2010),” “Front Page of Inpatient Medical Record (2011),” and “Basic Specifications for Electronic Medical Records (Trial) (2010)” formulated and promulgated by the former Ministry of Health of China.
Correspondingly, the National Administration of Traditional Chinese Medicine has formulated and promulgated the Basic Specifications for Writing Medical Records in Traditional Chinese Medicine, the Front Page of Inpatient Medical Records in Traditional Chinese Medicine (2011), and the Basic Specifications for Electronic Medical Records in Traditional Chinese Medicine (2010). Information from TCM operational specifications is reflected in the relevant sections of the Basic Data Set for Electronic Medical Records standard. Compared with the 2009 version of the electronic medical record data set, the structuring of TCM information has been improved to a certain extent.
III. Standardization of Electronic Medical Record Functions
In 2010, commissioned by the Department of Medical Administration of the former Ministry of Health, the Hospital Management Institute of the National Health and Family Planning Commission established the Electronic Medical Record (EMR) Pilot Office. Over the past seven years, the Hospital Management Institute has drafted and formulated all business specifications and management-related industry standards for EMRs, including documents such as the Basic Specifications for Electronic Medical Records, Functional Specifications for Electronic Medical Record Systems, Graded Evaluation Standards for the Application Level of Electronic Medical Record Systems, and Management Specifications for the Application of Electronic Medical Records.
Among these, the “Graded Evaluation of EMR System Application Level,” conducted based on the “Grading Evaluation Standards for EMR System Application Levels” (hereinafter referred to as the “Methods and Standards”), is the most well-known.
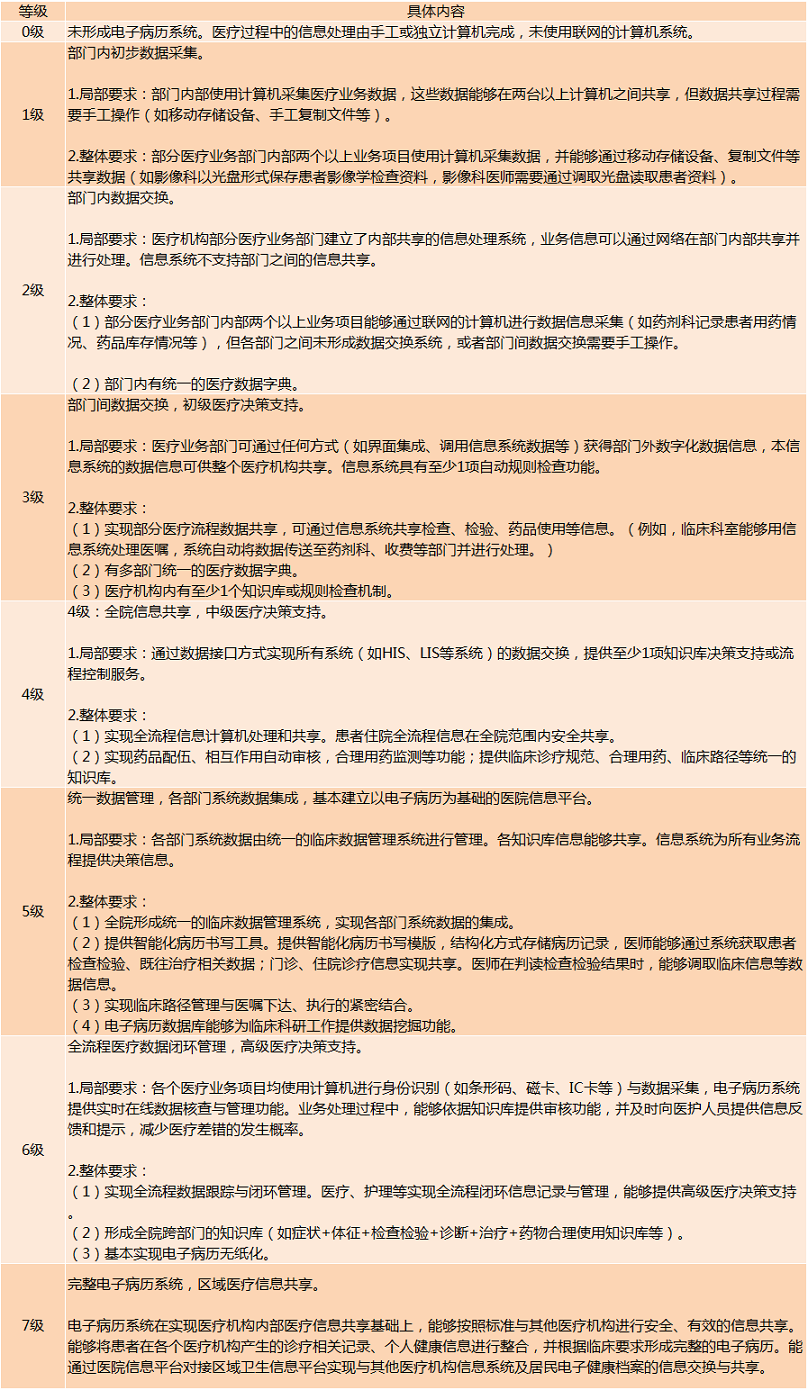
According to the "Methods and Standards," the application levels of electronic medical record (EMR) systems are classified into eight grades. The criteria for each grade include requirements for specific components of the EMR system as well as for the overall health information system.
Since 2011, the hospital research institute has self-funded the development of a data entry platform, conducted training on the construction of basic informatization capabilities in hospitals across China and promoted the implementation of relevant standards, and organized graded evaluations of electronic medical record (EMR) system application levels for secondary and tertiary healthcare institutions nationwide.
Over the six years since the evaluation initiative was launched, the Hospital Research Institute has conducted graded assessments of electronic medical record (EMR) system application levels for nearly 6,000 hospitals across China. Among these, secondary hospitals accounted for 52% of all secondary hospitals nationwide, while tertiary hospitals represented 80% of all tertiary hospitals in the country.
At the 2015 China Hospital Information Network Congress (CHINC), statistics were compiled on the current level of electronic medical record (EMR) adoption in hospitals. A total of 2,622 hospitals participated in the data submission. Among them, only 15 hospitals had reached EMR application level 5 or above, accounting for a mere 9‰. Hospitals implementing electronic signatures represented 20% of the evaluated institutions, with an average electronic signature application level of 2.99. These figures indicate that the application level of EMR systems in China remains very low.
 2015Only 6‰ of Hospitals in China Have Achieved EMR Level 5 or Above
2015Only 6‰ of Hospitals in China Have Achieved EMR Level 5 or Above
Appendix:2016 Level of Electronic Medical Record (EMR) Application in Hospitals

Data Source: China Digital Medicine
In 2006, the Healthcare Information and Management Systems Society (HIMSS) released《Electronic Medical Records vs. Electronic Health Records:Yes,There ls a Dif-ference》The white paper proposes the Electronic Medical Records Adoption Model (EMRAM) and uses it as a basis to evaluate the level of informatization in healthcare institutions.
The fundamental mission of HIMSS and HIMSS Greater China is to drive healthcare transformation through the adoption of information technology, optimize healthcare processes, and ultimately enhance patient safety and quality of care while improving the patient experience. The capabilities and proficiency in information technology are increasingly influencing hospitals’ capacities and performance in both clinical service delivery and operational management.
HIMSS evaluations focus on electronic medical record systems and consist of eight levels. Personalized medicine, evidence-based medicine, and evidence-based management all critically depend on the extensive and in-depth use of modern information technology.
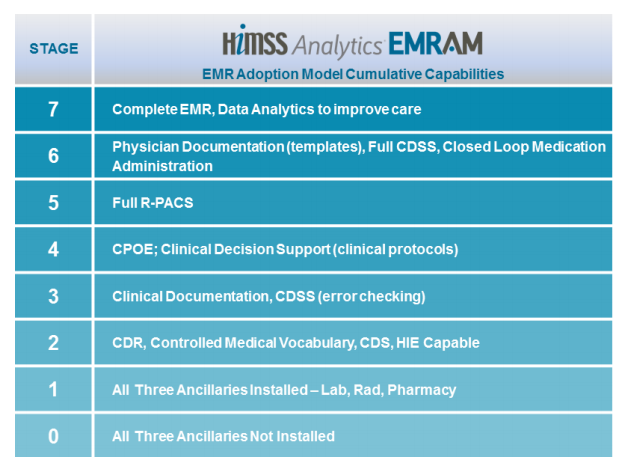 HIMSS EMRAM Rating System Levels Source: HIMSS Analytics Official Website
HIMSS EMRAM Rating System Levels Source: HIMSS Analytics Official Website
Based on feedback from hospitals and HIMSS’s research into the real-world impact of its rating consultancy, preparation, and review processes, the HIMSS EMRAM rating consultancy, preparation, and onsite review process can significantly drive hospital information technology development, primarily including:
(1) Assess the current level of construction and provide guidance for future development: The HIMSS EMRAM model summarizes the natural progression of hospital information technology adoption. It serves not only as an evaluation tool but also as a roadmap to guide the direction of hospital IT construction.
By leveraging this standardized model, which integrates Analytics rating data with on-site evaluations by experts during consultations and reviews, it is possible to accurately assess a hospital’s current stage of informatization development, its specific level of construction, and the areas requiring improvement.
Meanwhile, during the consultation, preparation, and review processes, the HIMSS EMRAM model can provide hospitals with a clear, reliable, and proven direction and pathway for development, enabling them to understand their current status, identify the right direction, determine the next steps, and clarify their ultimate goals.
(2) Provide a technical foundation for refined management and lay the groundwork for the hospital’s future refined management practices: Information technology is the technical prerequisite for implementing refined management in hospitals. During the consulting, preparation, and assessment processes for HIMSS EMRAM accreditation, which centers on clinical operations, hospitals focus on targeted promotion of information technology applications. This process will drive business process reengineering and optimization based on new technologies, thereby providing a technical foundation for the hospital’s transition to refined management.
Leveraging the roadmap functionality of the HIMSS EMRAM model, along with practical guidance from experts on business processes and technology applications during consultation, preparation, and review phases, hospitals can complete the reengineering or optimization of clinical systems and processes within a relatively short cycle. This lays the foundation for the future development and implementation of a more in-depth refined management system, serving, when necessary, as a pivotal milestone in the hospital’s transition from traditional management models to refined management practices.
(3) Assist hospitals in evaluating and enhancing their leadership and execution capabilities in informatization: The successful implementation and long-term sustainability of hospital informatization require the collective support and participation of all stakeholders, ranging from top-level decision-makers and middle management to the IT department, administrative staff, and frontline clinical personnel. The consulting, preparatory, and assessment processes associated with HIMSS EMRAM accreditation can targetedly, intuitively demonstrate, evaluate, and strengthen the informatization capabilities across all levels of the hospital, thereby facilitating the establishment and standardization of robust informatization practices.
For hospitals, the HIMSS EMRAM rating enhances capabilities across various dimensions. It serves as a summary of the natural progression of hospital information technology development, functioning both as an evaluation tool and as a roadmap to guide the direction of such initiatives.
Although the HIMSS rating evaluates the breadth and depth of modern health information technology adoption in hospitals, achieving HIMSS Stage 7 would be unimaginable without advanced management thinking and strong leadership. The verification process for HIMSS Stage 7 is extremely rigorous,only 3% in the United StatesHospitals Achieve Level 7 Accreditation。
Data from the HIMSS Analytics official website shows that,There are currently 31 hospitals in China (including Hong Kong, Macao, and Taiwan) that have passed HIMSS EMRAM certification, with 27 at Stage 6 and 4 at Stage 7.. Except for Ninghe County Hospital in Tianjin, which is a Grade II Class A hospital, all others are tertiary hospitals or above.
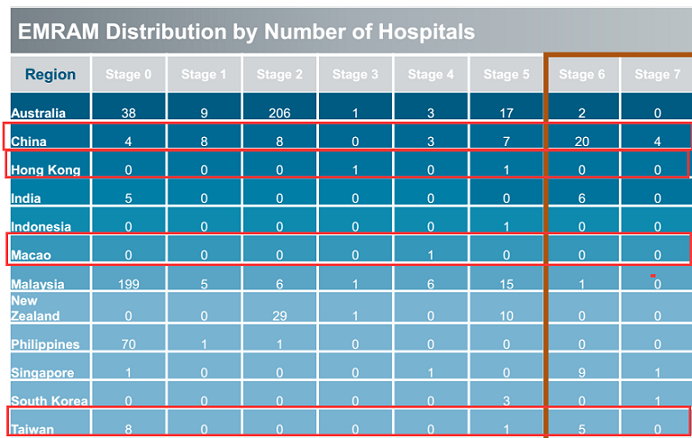 HIMSS EMRAM Adoption Status of Chinese Hospitals Source: HIMSS Analytics Official Website
HIMSS EMRAM Adoption Status of Chinese Hospitals Source: HIMSS Analytics Official Website
IV. Standardization of Interoperability for Electronic Medical Records
In September 2016, the National Health and Family Planning Commission consecutively issued three standards for medical informatization: the “Specification for Shared Documents of Electronic Medical Records,” the “Specification for Conformity Testing of Electronic Medical Records with Hospital Information Platform Standards,” and the “Specification for Conformity Testing of Electronic Health Records with Regional Health Information Platform Standards” (comprising a total of 57 health industry standards), explicitly stipulating that these standards would come into effect on February 1, 2017.
One of the 57 Health Industry Standards
Liu Jilan, Vice President of HIMSS and Director of Greater China, once mentioned that the development speed of electronic medical records in China is likely to surpass that of the United States.However, the strength of electronic medical records lies not in the number of subsystems, but in their ability to achieve interoperability.。
The standards released herein are based on the document architecture, providing normative specifications for the general structure of electronic medical record (EMR) sharing documents, and using template library constraints to normatively describe the specific business content of EMR sharing documents;Based on the basic data set of electronic medical records (EMR), this standard defines the data elements contained in EMR shared documents; using value domain codes as the standard, it normatively records coded data elements in EMR shared documents, clearly demonstrating the business context of specific application documents and the relationships between data units, thereby supporting higher-level semantic interoperability.
In addition to standardizing electronic medical records (EMRs), the national government has also focused on hospital information platforms centered on EMR systems and regional health information platforms centered on electronic health records (EHRs). It has issued the “Specification for Compliance Testing of Electronic Medical Records and Hospital Information Platform Standards” and the “Specification for Compliance Testing of Electronic Health Records and Regional Health Information Platform Standards.”
Among them, the *Specification for Conformity Testing of Standards for Electronic Medical Records and Hospital Information Platforms* specifies the conformity testing processes, methods, content, and criteria for determining test results related to hospital information interoperability standards. It is applicable to conformity testing of the basic data set standards for electronic medical records, conformity testing of the standards for shared document specifications for electronic medical records, and conformity testing of standards for hospital information platforms based on electronic medical records.
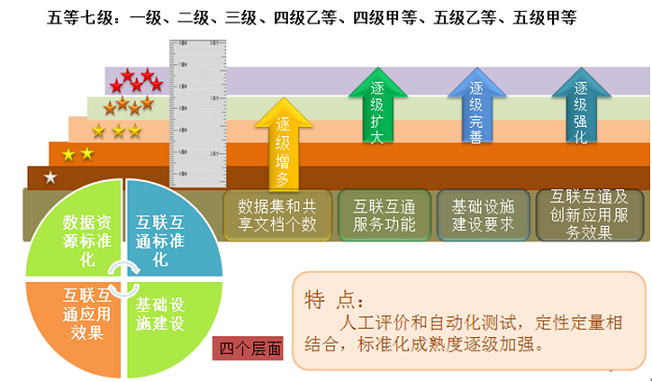
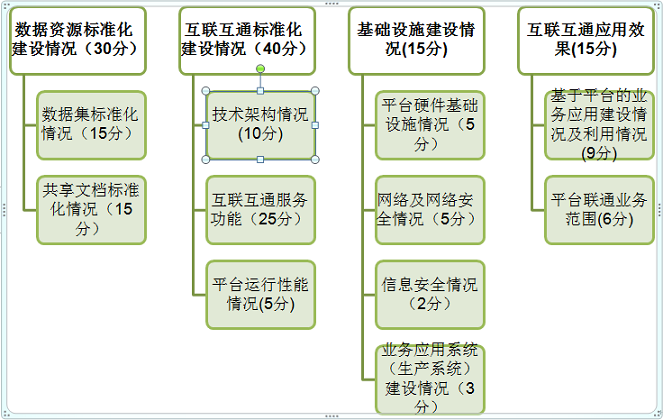
In December 2016, to further strengthen the promotion and application of health information standards, the Statistical Information Center of the National Health and Family Planning Commission (NHFPC), under the leadership of the Department of Planning and Information, organized and implemented the project for assessing the standardization maturity of interconnectivity in medical and health information. This initiative conducted comprehensive testing and evaluation of regional health information platforms and hospital information platforms across four dimensions: standardization of data resources, standardization of interconnectivity, infrastructure development, and the effectiveness of interconnectivity applications. By promoting utilization, improvement, and construction through assessment, the project aimed to facilitate cross-institutional and cross-regional interconnectivity and information sharing.
As an authorized third-party testing institution for the National Assessment of Standardization Maturity in Healthcare Information Interconnectivity, the China Software Testing Center is primarily responsible for laboratory testing, on-site quantitative indicator sampling for project application evaluations, and the preparation of comprehensive inspection reports. Leveraging the technical expertise accumulated through the national assessment of healthcare information interconnectivity standardization maturity, the Center also provides standards compliance testing services for medical business systems related to electronic medical records and health business information systems related to health records, in accordance with relevant health industry standards.
Assessment Content
The National Health and Medical Information Interconnectivity Standardization Maturity Assessment comprises two phases: laboratory testing and project application evaluation. The laboratory testing indicator system consists of three components: data resources, interoperability, and technical architecture. The project application evaluation indicator system is illustrated in the figure below.
Assessment Process
V. Standardization of Electronic Medical Record Management and Use
In 2013, the National Health and Family Planning Commission issued the Provisions on the Administration of Medical Records in Medical Institutions (2013 Edition), which clearly specified requirements for the establishment, custody, borrowing and copying, and retention of medical records. Article 6 of the General Provisions states that medical institutions and their medical personnel shall strictly protect patient privacy and are prohibited from disclosing patients’ medical record data for purposes other than medical care, teaching, or research. Therefore, the use of electronic medical records should be limited solely to medical care, teaching, and research; any other use constitutes a regulatory violation.
In February 2017, the National Health and Family Planning Commission promulgated the new “Administrative Specifications for the Application of Electronic Medical Records (Trial)” (hereinafter referred to as the “Specifications”).
The official notice accompanying the new edition of the Standards explicitly emphasizes promoting the effective sharing of electronic medical records (EMRs). Article 8 of Chapter II stipulates that, under the premise of ensuring information security, the effective sharing of EMR data shall be facilitated. This provision was not included in the previous edition of the Standards.
Furthermore, there are also some changes to the copyable objects of patients’ electronic medical records in the new version of the Specifications.
Article 26 of the previous version of the Specifications stipulates that medical institutions shall accept applications for photocopying or reproducing electronic medical record data from the following individuals or entities:
(1) The patient themselves or their agent;
(2) Close relatives of the deceased patient or their agents;
(3) Basic medical insurance management and handling agencies that pay expenses for patients;
(4) Insurance institutions authorized by the patient.
However, the new version of the Regulations does not mention insurance institutions or basic medical security management and handling agencies. Instead, Article 21 only stipulates that medical institutions shall provide applicants with copying services for electronic medical records. Medical institutions may provide medical records in either electronic or printed format.
Medical institutions with the necessary capabilities may provide patients with electronic copies of medical imaging scans, surgical recordings, and interventional procedure videos.
The narrowing scope of replicable objects indicates that the National Health and Family Planning Commission has imposed stricter restrictions on the privacy of electronic medical records (EMRs). Consequently, medical consortia and patients themselves are likely to become the core channels for EMR sharing and utilization. Furthermore, the enhanced level of EMR sharing presents a clear benefit to the development of big data in healthcare.
Article 11 of the previous version of the "Specifications" states: The electronic medical record system shall establish a personal information database for each patient (including name, gender, date of birth, ethnicity, marital status, occupation, employer, address, valid identity document number, social security number or health insurance number, and contact telephone number), assign a unique identifier, and ensure its correspondence with the patient's medical records.
Article 13 of the revised "Specifications" has amended this sentence to read: "Medical institutions shall assign a unique patient identity identifier to each patient's electronic medical record, so as to ensure the authenticity, consistency, continuity, and completeness of the patient's basic information and medical records."
One aspect corresponds to traditional medical records, while the other explicitly establishes electronic medical records (EMRs) as the unique patient identifier, underscoring their heightened importance. Furthermore, emphasis is placed on the authenticity, consistency, continuity, and completeness of medical records, which serve as the foundational guarantee for the big data application of EMRs.
Summary
With the continuous improvement of electronic medical record (EMR) standardization, health IT vendors, big data firms, and artificial intelligence companies are brimming with development opportunities. Enterprises should continuously enhance their existing systems and closely collaborate with frontline clinical healthcare professionals. On one hand, for large tertiary hospitals, efforts should focus on deepening and broadening EMR applications, improving integration with other information systems, and meeting the specialized needs of various clinical departments.
On the other hand, enterprises should closely align with clinical management and diagnostic and treatment workflows to make their products better suited to hospital needs. Meanwhile, they should pay close attention to national and local regulations, standards, and policy guidelines, emphasizing the application of standards and specifications to ensure system interoperability, thereby adapting to the future trend of regional health information sharing and the establishment of electronic health records for residents.