What Kind of Training Do Grassroots Doctors Need? Medical Technology, Marketing, and More
By Che Feilun, General Manager of Shenzhen Kehengli Computer Software Co., Ltd.
The key to tiered diagnosis and treatment lies in strengthening primary care by enhancing the clinical skills and service capabilities of primary care physicians, which has gradually become an industry consensus.
There is a large workforce in primary healthcare institutions, with over one million village doctors alone. Although primary care physicians—especially village doctors—play a unique and vital role, they have long been working in remote rural areas. Burdened with tedious grassroots tasks and lacking access to learning opportunities, they exhibit varying levels of medical expertise. The high susceptibility to medical accidents leaves them walking on thin ice.
Primary care physicians have a strong demand for adopting new technologies and therapies, as well as for improving compensation and doubling their income. So how can these demands be met?
Numerous Challenges at the Primary Care Level: The Best Fit for Physicians Is What Matters Most
There are numerous issues affecting primary care physicians, particularly rural doctors. For instance, there is a conflict between maintaining clinical practice and suspending work for training: since primary care physicians operate on a self-financing basis, with the government providing only a modest subsidy for disease prevention and control, any suspension of practice for educational purposes directly impacts their income. Furthermore, the proliferation of various training fees and bundled charges discourages primary care physicians from participating in training programs. Additionally, the medical income of some primary care physicians is insufficient to sustain their household expenses, making it impractical to require them to leave their posts for off-site training or to expect busy medical specialists to frequently conduct on-site training at the grassroots level.
Most training programs currently available on the market are poorly structured and lack specificity: they place excessive emphasis on the use of sophisticated high-end equipment, surgical interventions, and the application of costly new specialty drugs, all of which are unsuitable for primary care settings.
In the context of a comprehensive tiered diagnosis and treatment system (featuring two-way referrals and separate management of acute and chronic conditions), it is imperative to establish systematic training tailored to primary care. Since clinics do not necessarily require highly specialized physicians but rather practitioners capable of managing common, general, and chronic diseases, training curricula should align closely with the expectations of primary care physicians. Emphasis should be placed on practicality, hands-on application, and operability, enabling these physicians to acquire medically valuable, pragmatic skills. In contrast, the content of traditional continuing medical education is often perceived as overly abstract and inaccessible.
Nowadays, grassroots physicians have a greater need for standardized residency training that is practical, substantive, and communicated in plain language. This should be considered primarily from the following aspects:
1. Primary healthcare institutions (particularly village clinics) have limited equipment; therefore, courses on using equipment to assist in disease diagnosis and treatment should focus on the devices currently available at these primary care facilities as the core technical content.
2. Pay close attention to integrating new policies and emerging trends, ensuring that primary care physicians fully understand current policy updates, acquire novel and practical appropriate technologies for primary care, reflect the distinctive characteristics of their roles, and deliver services that address every detail of people’s daily lives;
3. Appropriate technologies for primary care have three characteristics: First, universality—they can be applied to a wide range of common, frequently occurring, and chronic diseases, are easy for general practitioners to master, and require few additional conditions for use. Second, effectiveness—they provide tangible benefits to primary care physicians in the diagnosis, treatment, rehabilitation, and prevention of diseases. Third, affordability—the costs are relatively low, making them suitable for the financial capacity of the majority of the population.
Use Clinical Decision Support Systems to Train General Practitioners and Reduce Training Time
Premier of the State Council Li Keqiang stated, “Retaining village doctors is more effective than building large hospitals.” Professor Wang Xiaoning, Director of the Geriatrics Institute at the Chinese PLA General Hospital and Vice Chairman of the Tiered Diagnosis and Treatment System Engineering Professional Committee under the China Association for Promotion of Rehabilitation Technology Transformation and Development, pointed out: “It is unrealistic and unreliable to expect that training a large number of general practitioners will solve national health problems by having GPs, who have undergone more than ten years of education, work at the grassroots level.” This indicates that factors such as vested interests and technological asymmetry make it neither feasible nor necessary for physicians from secondary Grade A (Er Jia) and tertiary Grade A (San Jia) hospitals to move to grassroots institutions. The transformation of grassroots doctors into general practitioners is imminent. Gradually transitioning into licensed (assistant) physicians and general practitioners is undoubtedly the inevitable path for China’s more than one million village doctors.
For primary care physicians to become qualified general practitioners, they must have a thorough command of common diseases across various medical specialties. General practitioners can be described as “generalists” in the medical field, requiring proficiency in internal medicine, surgery, obstetrics and gynecology, pediatrics, neurology, and other disciplines. What kind of “training” is required for primary care physicians to become family general practitioners?
Training a general practitioner under the “Standardized Residency Training” model takes 5 to 10 years. However, obtaining the qualification of Rural General Practice Assistant Physician and leveraging effective intelligent diagnostic and therapeutic assistance technologies can reduce the training period by more than three years. With the aid of “Kehengli Prescription and Medical Record Software—Becoming a Doctor with Ease” and the “Intelligent Clinical Diagnosis and Treatment System,” primary care physicians can readily acquire general practice competencies, enhance their diagnostic and treatment capabilities, and improve work efficiency. Consequently, it is not difficult for them to achieve the proficiency level of general practitioners in managing minor illnesses, common diseases, frequently occurring conditions, and the remission phases of chronic diseases (previously diagnosed and examined at major hospitals).
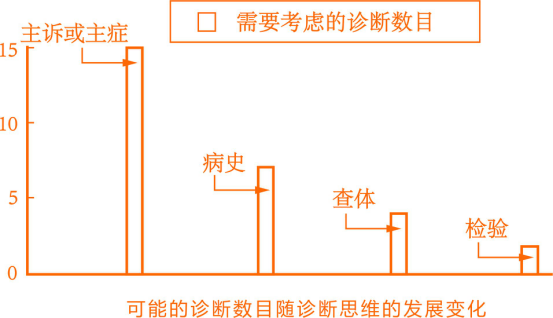
To enhance clinical diagnostic proficiency, draw inferences from one instance to others, and achieve twice the result with half the effort in clinical practice, it is essential to master and apply scientific thinking methods. The extent and efficiency of applying clinical reasoning directly reflect a clinician’s ability and competence in recognizing and managing diseases. As the largest clinical reasoning training platform in China with a simulated case library, Zhiqu first presents all findings from history taking, physical examination, laboratory tests, and special examinations, or retains only pathological results with definitive diagnostic value, before proceeding to analysis and diagnosis. This approach, characterized by “applying diagnostic reasoning only after complete data are available,” is particularly suitable for standardized residency training.
As a clinical intelligent diagnosis and treatment system that emulates physicians’ thinking, every step—from initial patient contact, history taking, and physical examination to laboratory tests and specialized investigations, culminating in a final diagnosis—is guided by the reasoning process of “hypothesis-driven diagnosis and diagnostic verification.” It does not merely apply diagnostic reasoning after all data have been collected to arrive at a diagnosis. The “stepwise narrowing of diagnostic possibilities” approach it embodies is particularly suitable for primary care physicians, especially rural doctors, who often lack access to laboratory and specialized testing, thereby helping them train their clinical reasoning skills.
Specialized Departments: Enhancing Outpatient Competitiveness
Many patients are not unwilling to seek care in community settings; rather, they often lack familiarity with primary care physicians and do not trust “jack-of-all-trades” doctors—who create the impression of being able to treat everything yet fail to effectively manage any specific condition, thereby forfeiting the sharpest tool in marketing: precise market positioning. Instead, these patients tend to place their trust exclusively in specialists with focused expertise.
The renowned speaker Brian Tracy once said: “Anyone who focuses on a single field can become an expert in five years, an authority in ten years, and a world-class leader in fifteen years.” Most physicians are unwilling to make trade-offs or let go, which prevents them from maintaining focus; consequently, it is difficult for them to become specialists in specific diseases. As the old oil seller remarked, “There is no secret to my skill—only practice makes perfect.”
Take a look at primary care clinics and community health stations: the most sought-after physicians are still those specializing in specific diseases and specialties, with annual incomes reaching hundreds of thousands of yuan exclusively found in specialized outpatient clinics offering distinctive treatments. Therefore, for general practitioners, leveraging intelligent diagnostic systems to assist in diagnosis and save time, while focusing on specialized disease areas, is undoubtedly the path to breaking through in primary care.
As operators of primary care outpatient clinics and health stations, it is essential to fully recognize that “serving the community” is the foundation, while “differentiated development” is the core business philosophy. Guided by the principle of “offering what others do not, and excelling where others merely participate,” practitioners should continuously enhance their medical expertise, leverage unique technical advantages to boost clinic competitiveness, and better serve the general public. *Secrets to Success in Primary Care* and specialized, highly effective clinical techniques can guide primary care physicians in establishing distinctive and high-efficacy specialty practices, achieving the goal of “definitive cure upon treatment,” building personal brands, and multiplying income.
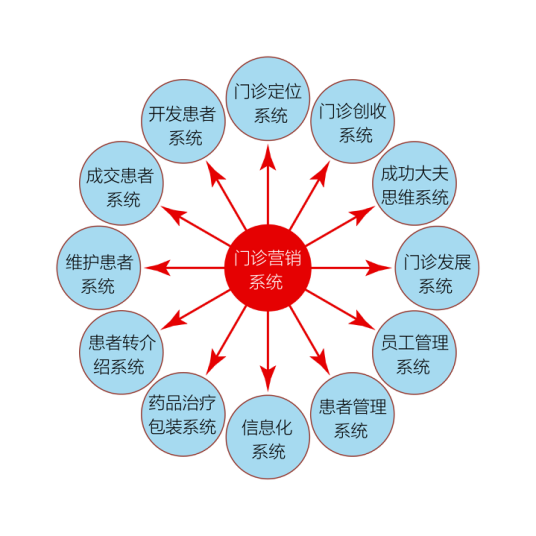
Marketing Technology: Doubling Revenue, Building Brands
If primary healthcare institutions fail to learn self-branding and self-marketing, and leverage their soft power, it will be difficult to truly direct patients to the primary care level, relying solely on tilted medical insurance reimbursement ratios and ineffective medical consortia.
“Secrets to Success in Primary Care” is also a toolkit designed to help primary care institutions rapidly generate profits in the healthcare industry. It aims to introduce strategies for reallocating medical resources with low investment and low risk, leveraging a series of innovative technologies to multiply revenue for primary care institutions.
Promote Characteristic Appropriate Technologies of Traditional Chinese Medicine
At present, the state is heavily investing in primary healthcare. As an important component of the health sector, Traditional Chinese Medicine (TCM) occupies a significant position in primary healthcare services due to its unique advantages of being “simple, convenient, effective, and affordable.” With changes in lifestyles and work patterns, the social issues of “difficulty in accessing medical care” and “high medical costs” have become increasingly prominent. Currently, the difficulty in accessing medical care is not only evident in large cities and major hospitals but is even more pronounced in remote areas. The primary reason for this is the long-term concentration of medical resources in large hospitals, while community and primary healthcare institutions have failed to play their intended roles.
In China, primary community healthcare still faces a series of challenges, including outdated equipment, insufficient technical proficiency among practitioners, suboptimal service quality, restrictions on the use of essential medicines, and policies limiting antibiotic and intravenous drip usage. These issues have made the operation of primary healthcare institutions increasingly difficult. Therefore, developing a primary traditional Chinese medicine (TCM) healthcare model centered on appropriate TCM technologies is an effective approach to resolving this contradiction.
Primary care physicians well understand the principle that administering medication is akin to deploying troops. As a distinctive and appropriate Traditional Chinese Medicine (TCM) technique, acupoint application therapy is safe, reliable, and reduces the need for oral medications and injections (especially as most primary healthcare institutions have implemented restrictions on intravenous drips). Thermal Pulsating Moxibustion, as a novel acupoint application product, offers unique therapeutic efficacy by integrating moxibustion, thermotherapy, and pharmacotherapy into a single treatment. It avoids risks associated with injections and oral drug allergies, helps prevent medical accidents and bodily harm, and does not burden the liver or kidneys. Just as humanity needs green food and a green environment, it also requires green healthcare—Thermal Pulsating Moxibustion.
Training Mode: Offline Promotion + Live Streaming
Patients follow their doctors’ advice. Physicians are the core of healthcare and its most scarce resource. From the perspective of entrepreneurship in the medical industry, whether “online” or “offline,” any venture without a cohort of high-quality, highly engaged physicians is merely theoretical.
Precisely because physicians constitute a specialized demographic that is skeptical of advertising and accustomed to face-to-face interactions, on-the-ground promotion teams are essential for effective marketing. By continuously funneling physicians acquired through offline marketing into the “encirclement” of new media marketing, organizations can integrate online and offline strategies, allowing them to reinforce each other and jointly breach market barriers.
From a formal perspective, we recognize that while internet-plus models may not be well-suited for disease diagnosis and treatment, they are highly suitable for training and education, with internet-plus training being readily implementable. Xing Shuai believes that “traditional school-based education emphasizes theory over practical application, making it difficult for students to acquire mature, job-ready skills in an academic setting. Consequently, the societal demand for skill-oriented competencies highlights the shortcomings of traditional education and underscores the importance of skills development. Online skill-based instruction precisely meets this need.”
Overall, primary care physicians have limited opportunities for learning, especially for off-site training, despite the extensive content available. Live streaming can effectively address this issue. For training providers, leveraging internet-based methods can enhance the efficiency of delivering training programs.
For instance, offering a free training session might attract only a few hundred to a few thousand attendees in person (even with travel subsidies), whereas leveraging live streaming (in the evening) can enable tens of thousands, or even more, to simultaneously access the highly interactive training content.
The number of primary healthcare institutions far exceeds that of hospitals. Given the current landscape characterized by small scale, fragmentation, disorganization, and uneven quality, entrepreneurs must identify an appropriate entry point from the outset. For instance, as offline ground-promotion costs continue to rise, it is advisable to embed paid products such as Thermal Pulse Moxibustion—which align with “rigid demand,” “pain points,” and “high-frequency” usage—into complimentary training services, thereby avoiding premature failure before gaining traction.
Stay tuned for the next article: Brand Building in the Primary Healthcare System