Comprehensive Research on AI in Medical Imaging Diagnosis: Excerpt from the 2017 Healthcare Big Data and Artificial Intelligence Industry Report
2Since 2016, the global consensus has been that the inflection point for artificial intelligence has arrived. From world-class players like Google and IBM to fervent investors and entrepreneurs, all are racing to secure strategic positions, even engaging in an AI arms race. Artificial intelligence is experiencing a surge in prosperity worldwide.
How should we view and think about this surging wave of artificial intelligence? As a witness to this tide, VCBeat is compelled to leave its mark on it.
VCBeat·VBInsight’s 2017 flagship publication—“2017 Industry Report on Medical Big Data and Artificial Intelligence”—will be released on September 16 at the Forum on Industrial Practices in Healthcare Big Data and Artificial Intelligence.
This comprehensive report, totaling 100,000 words, was compiled by VCBeat over the course of one month, following a review of more than one million words of source materials and interviews with senior executives from dozens of artificial intelligence companies. It represents VCBeat’s most systematic analysis to date of the AI in healthcare sector, providing a detailed examination of the underlying technologies of medical big data and AI enterprises, nine key subsectors of medical AI, and the current landscape of medical AI companies, while also featuring case studies of more than 60 domestic and international firms.
Meanwhile, VCBeat’s VBInsight attempts to objectively describe the development status of various subsectors within AI + healthcare using our proprietary methodology. We have compiled data on financing and investment activities for a total of 192 medical AI companies both domestically and internationally, and for the first time, we have mapped out the technology maturity curve for subfields of AI in healthcare to serve as a reference for industry professionals.
There are two ways to obtain the full report:
I. Register to attend the 2017 Yangtze River Industry Forum (Autumn) and the Conference on Big Data and Artificial Intelligence in Healthcare, held on September 16–17,Click to Register),Obtain a printed copy of the full report, review the list of AI healthcare companies and understand the current development status across various sectors.
2. Scan the QR code below to become an official VCBeat member, and you will receive the complete electronic version of the "2017 Medical Big Data and Artificial Intelligence Industry Report" after its official release on September 16.

The following is a curated serial excerpt from the report; the full version contains much more comprehensive content.
Medical Big Data and Artificial Intelligence Industry Report II:Medical Imaging Section
Modern medicine is evidence-based medicine founded on experimental research. Physicians’ diagnostic and treatment conclusions must be grounded in corresponding diagnostic data, with medical imaging serving as a critical diagnostic basis. Indeed, 80%–90% of healthcare data originates from medical imaging. Consequently, clinicians have substantial demand for imaging capabilities, requiring various quantitative analyses of medical images and comparisons with historical images to arrive at a diagnosis.
“AI + Medical Imaging” refers to an auxiliary tool that leverages deep learning algorithms on medical images to perform tasks such as image classification, object detection, image segmentation, and retrieval, thereby assisting physicians in diagnosis and treatment.
I. Modes of Artificial Intelligence Participation in Medical Imaging Diagnosis
Our AI capabilities in image processing are categorized into four types: image classification, object detection, image segmentation, and image retrieval.
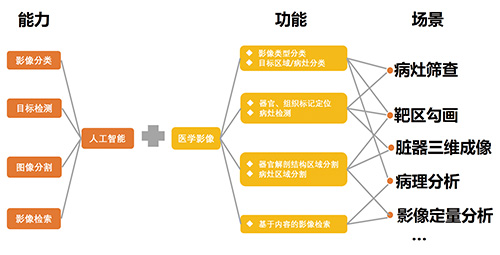
Medical Imaging + Artificial Intelligence: Primary Operational Models
We take liver disease screening as an example to illustrate how artificial intelligence participates in medical imaging:
The primary step for artificial intelligence to participate in the medical process is to acquire a large volume of annotated medical imaging samples, and then attempt to identify key points within them. For instance, this involves locating points near the lungs and liver. After identifying these key points, an initial model is established by incorporating shape priors of the liver. Subsequently, machine learning techniques are employed to learn the characteristics of boundaries and lesions, striving to approximate boundary information as closely as possible. The model is further refined using shape features, ultimately yielding high-quality segmentation and screening results. This process constitutes the localization, classification, and segmentation of images by artificial intelligence.
After segmenting organs and annotating lesions, we can determine whether a specific region is affected by disease, but we cannot identify the specific pathology or assess the severity of disease progression. At this stage, analysis of pathological images is required to obtain evidence for auxiliary diagnosis.
Pathological analysis is a diagnostic method that involves extracting living tissue from suspected lesions and analyzing cellular morphology under a microscope; it is currently the primary means of confirming cancer diagnoses. Digital pathology images are often extremely large, with some tumor pathology images reaching dimensions of 200,000 × 200,000 pixels, or even 400,000 × 400,000 pixels, containing a vast number of cells requiring analysis. This represents an enormous analytical burden, requiring physicians to spend considerable time on comparison and evaluation. As the amount of information contained in pathology images continues to increase, relying solely on physicians for this task has become increasingly impractical.
By constructing neural networks and leveraging deep learning algorithms, artificial intelligence systems undergo extensive training on pathological databases containing cells with various morphological lesions, thereby acquiring the ability to recognize characteristics of diseased cells. Utilizing the aforementioned segmentation algorithms, individual cells are isolated; through comprehensive comparative analysis, the system identifies the type and progression stage of cellular lesions, providing auxiliary evidence to support physicians in making final diagnoses.
Approximately 85% of the storage capacity in hospital big data systems is occupied by imaging data. Current computers can recognize structured text data and structured imaging data, and are exploring methods to integrate functional medical images with structural images to achieve better diagnostic and therapeutic outcomes. By combining these four capabilities, specific application scenarios for artificial intelligence in medical imaging are realized.
II. Changes Brought by Artificial Intelligence to Medical Imaging

Differences Between Traditional Methods and AI-Based Image Interpretation
III. Applications of AI + Medical Imaging Across Various Fields
Currently, the main applications of artificial intelligence in medical imaging fall into three categories: disease screening, lesion segmentation, and 3D organ imaging. We have summarized the primary approaches AI employs in medical imaging as well as the most commonly used imaging modalities. In the following sections, we will provide a detailed overview of AI applications in some of the most prominent areas, including lung cancer screening, diabetic retinopathy screening, lesion segmentation, 3D organ imaging, and pathological analysis.
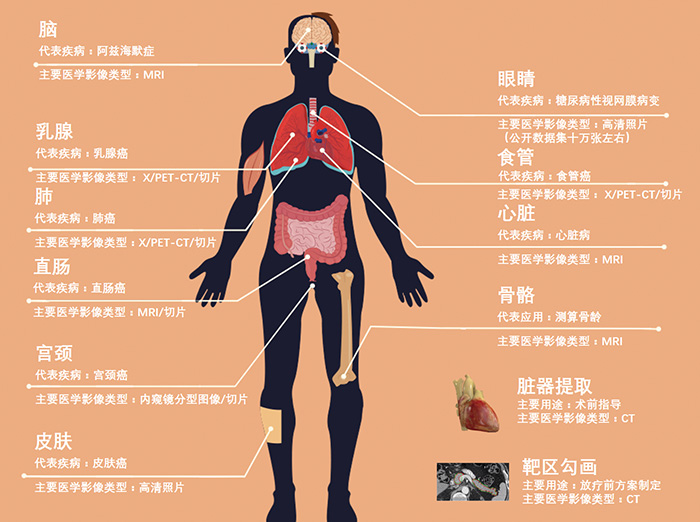
The Current Role of Artificial Intelligence in Human Medical Imaging Examinations

The steps for AI-based lung screening are as follows: First, an image segmentation algorithm is applied to process lung scan sequences to generate lung region maps, from which lung images are derived. Using the lung region images obtained from segmentation, along with nodule annotation data, nodule region images are generated to train a convolutional neural network (CNN)-based pulmonary nodule segmenter. This segmenter is then used to perform pulmonary nodule segmentation on the images, yielding regions of suspected pulmonary nodules. Once suspected nodules are identified, a 3D convolutional neural network is employed to classify them, thereby determining the locations and confidence levels of true pulmonary nodules.
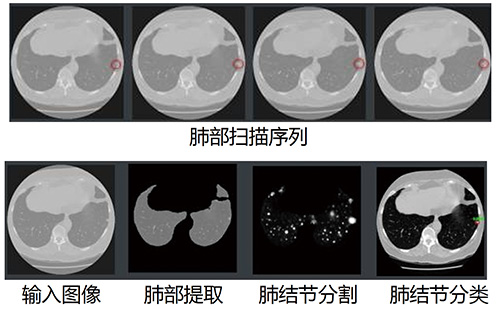
Imaging Screening for Pulmonary Diseases
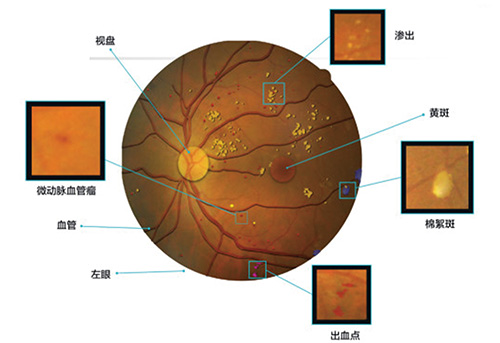
# Main Symptoms and Examination Points of Diabetic Retinopathy
Diabetic retinopathy, abbreviated as "DR," is a common retinal vascular disease and the leading cause of blindness among patients with diabetes.
Because diabetic retinopathy often presents no clinical symptoms in its early stages, by the time symptoms appear, the condition has usually progressed to a severe stage, making it easy to miss the optimal window for treatment. Therefore, the efficacy of treatment for diabetic retinopathy depends on timeliness. However, due to a shortage of ophthalmologists and low public awareness in China, the current screening rate for diabetic retinopathy remains below 10%.
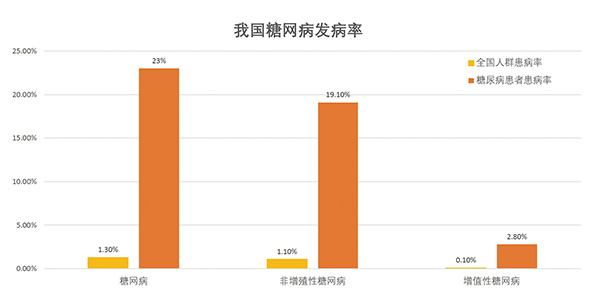
Statistics on the Incidence of Diabetic Retinopathy in China
Screening for diabetic retinopathy has not been widely implemented, partly due to the shortage of physicians relative to the large patient population, and partly due to certain objective challenges:
1. The patient population with diabetic retinopathy is large and growing rapidly, while the adoption rate of fundus imaging devices falls far short of meeting demand. However, due to the high cost of these devices, large-scale procurement remains impractical for underdeveloped regions.
2. With growing public awareness of diabetic retinopathy screening and national policy support, the demand for fundus image interpretation is rising. The current number of ophthalmologists is insufficient to handle this workload, leading to physician burnout and an increased incidence of misdiagnosis and missed diagnoses. Furthermore, experienced physicians are reluctant to devote their time exclusively to image reading, as they prefer to allocate more time to research and generating new findings. This has further exacerbated the shortage of medical professionals.
3. The training of physicians engaged in fundus image interpretation is slow and inconsistent, leading to variability in readings among different doctors and resulting in a lack of quantitative information in diagnostic outcomes.
4. Data management and analysis for fundus image reading are highly challenging. Currently, data is simply archived, but the substantial workload required for data organization makes it difficult to reuse the reading data.
5. Patients with diabetes often face mobility challenges due to advanced age or systemic multi-system complications, live far from medical institutions with adequate ophthalmic service capabilities within their region, and experience prolonged waiting or examination times at these facilities.
These pain points are primarily caused by an imbalance between the supply and demand of medical services. Since image recognition is a specialty of artificial intelligence (AI), leveraging AI for preliminary screening will significantly improve the current state of diabetic retinopathy screening.
Currently, the following nine companies are utilizing AI for diabetic retinopathy screening:

AI Company for Diabetic Retinopathy Screening
Target volume delineation and treatment planning consume a significant amount of oncologists' time.
Most patients experience significant panic upon being diagnosed with a tumor, consulting their physicians at the slightest physical change or symptom. However, oncology departments in renowned Grade A tertiary hospitals are typically overcrowded. In addition to clinical duties, physicians bear responsibilities such as scientific research. Consequently, they may become frustrated when faced with relentless questioning from patients.
Oncologists at primary healthcare institutions often lack experience, making them hesitant to formulate treatment plans for patients and leading to frequent referrals. This, in turn, exacerbates the tension between doctors and patients at tertiary hospitals. Therefore, hospitals are highly concerned with leveraging new technologies to improve physicians’ efficiency and enhance the treatment capabilities and confidence of primary care providers. In the process of cancer treatment, two tasks consume a significant amount of doctors’ time and energy: target volume delineation and treatment plan design.
Radiotherapy is the most mainstream of the three major cancer treatment modalities (the other two being surgery and chemotherapy). Compared with diagnosis, treatment lies closer to the core of medical care. Each cancer patient typically has around 200 CT images. During contouring, physicians must annotate the organs and tumor locations on each image. Using traditional methods, this process takes physicians 3–5 hours. After identifying the tumor location, physicians must also design a specific radiotherapy plan or surgical approach based on the tumor’s size, shape, and other characteristics, which includes assigning different radiation doses to different anatomical regions.
If all goes well, the patient is treated according to the doctor’s initial plan, shows improvement, and ultimately recovers. However, things do not always go as planned. In some cases, the first course of treatment proves ineffective (with less than a 30% reduction in tumor tissue) due to inaccurate delineation of the target volume or changes in the tumor. In such situations, the treatment plan needs to be revised, requiring the physician to re-delineate the targets and develop a new plan for the patient.
Intelligent Target Volume Delineation Software Interface
In our country, the average waiting time for cancer patients is two to three weeks. When a doctor spends time with one patient, another must continue to wait, which may result in missing the optimal treatment window.
Target delineation and treatment planning require technical expertise and clinical experience; however, they involve substantial repetitive tasks. These labor-intensive processes are well-suited for artificial intelligence, and leveraging AI to perform them can save oncologists significant time.

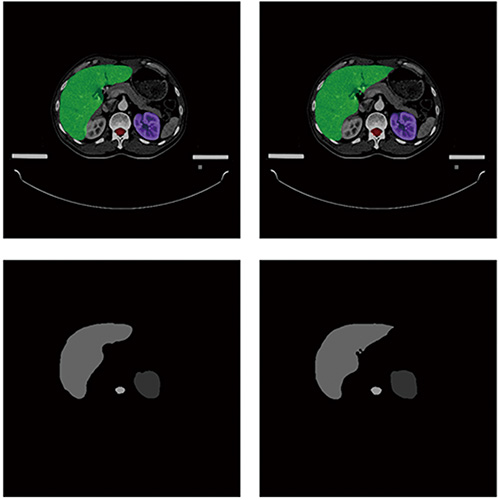
3D Organ Imaging VR Demonstration
3D Organ Imaging is an AI-driven technology that performs localization and segmentation of target organs based on medical imaging data, such as MRI and CT scans, to visualize the patient’s internal anatomy on a computer. By inputting the patient’s MRI, CT, and other diagnostic imaging data, the system renders a detailed view of the internal structures. As the surgeon points with a probe, the system updates the display in real time, providing clear visibility of anatomical positions, thereby making surgical procedures faster, more precise, and safer.
Automatically reconstructs realistic 3D models of organs, enabling physicians to directly observe the anatomical details of patients' true human structures from all angles within an augmented reality virtual space using specialized equipment. Through gesture and voice controls, users can perform real-time three-dimensional geometric analysis of organs and lesions, precisely measuring parameters such as location, volume, diameters, and distances of target structures. Additionally, the system supports virtual dissection, simulated surgical resection, surgical planning, and surgical risk assessment.
Even among rigorously trained pathologists, diagnostic discrepancies for the same patient exist, and such variability is a significant contributor to misdiagnosis. For instance, inter-rater agreement among physicians in diagnosing certain forms of breast and prostate cancer can be as low as 48%.
It is not surprising that physicians exhibit inconsistency in their practice, as making an accurate diagnosis requires them to interpret vast amounts of diagnostic data. Typically, pathologists are responsible for examining all biological tissues visible on pathology slides. However, each patient may have numerous slides, and at 40x magnification, each slide contains over 10 gigapixels (10+ gigapixels). Imagine having to review more than 1,000 megapixel images while being accountable for every single pixel. This entails processing enormous volumes of data, yet physicians often lack sufficient time to do so.
To address the challenges of limited time and diagnostic accuracy, integrating artificial intelligence (AI) into digital pathology research has emerged as the optimal solution. AI can reduce the time required for pathological diagnosis, enhance diagnostic efficiency, and, most importantly, deliver more accurate diagnostic results. The effective use of AI can genuinely assist pathologists in improving their interpretive capabilities, thereby enabling precision medicine through precise diagnosis.
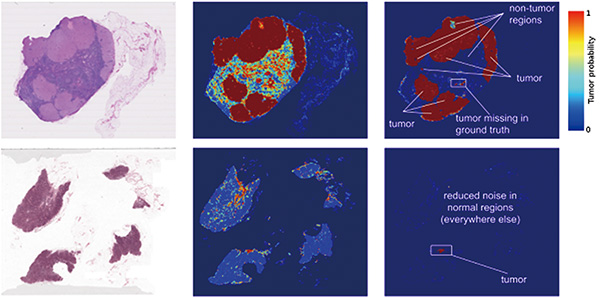
AI Detection of Tumor Pathology Image Results
The involvement of artificial intelligence has brought revolutionary changes to digital pathology research. Google has announced its use of deep learning algorithms to assist pathologists in determining whether pathological images depict breast cancer that has metastasized to the lymph nodes or breast cancer that has extended into adjacent breast tissue.
Currently, multiple enterprises in China have introduced artificial intelligence into pathological research.
IV. Research on AI Medical Imaging Companies
We conducted a comprehensive survey of the current operational status of AI medical imaging companies, resulting in the table below. This table fully reflects the data sources, data volume, and clinical implementation status of these AI companies. However, as each company is at a different stage of development and employs distinct market strategies, this data serves only to illustrate industry trends and is not suitable for comparative analysis.
(Please refer to the report for detailed tables.)
The survey data in the table are as follows:
True Positives: The number of cases identified as diseased (positive) by the technology under evaluation and also confirmed as diseased by the gold standard (denoted as a).
False Positive: The number of cases identified as diseased (positive) by the technology under evaluation but classified as disease-free (negative) by the gold standard (denoted as b).
False Negatives: The number of cases classified as disease-free (negative) by the technology under evaluation but as diseased (positive) by the gold standard (denoted as c).
True Negative: The number of cases determined to be disease-free (negative) by the technology under evaluation and also confirmed as disease-free by the gold standard (denoted as d).
Based on the above four values, the sensitivity, specificity, negative predictive value, and positive predictive value of this method can be determined.
Sensitivity = a/(a+c)
Sensitivity, also known as the true positive rate, reflects the missed diagnosis rate of a method in identifying a specific lesion. Sensitivity is generally expressed as a percentage; the higher the sensitivity, the lower the missed diagnosis rate. Methods used for screening a particular disease must have high sensitivity to minimize missed diagnoses.
Specificity = d/(b+d)
Specificity, also known as the true negative rate, reflects the false-positive rate of a method in diagnosing a specific lesion. Specificity is generally expressed as a percentage; the higher the specificity, the lower the false-positive rate. Screening methods for a particular disease do not necessarily require extremely high specificity, as long as it falls within an acceptable range.
From the current development perspective, companies attach great importance to clinical data and utilize it in model training. Even if public datasets are used for initial model training during the early startup phase, companies gradually align more closely with clinical practice as they grow.
Currently, regardless of the company or the disease involved, their systems all achieve a sensitivity rate exceeding 90%, a metric that physicians prioritize most. Poor sensitivity may result in failure to detect suspicious nodules, potentially exposing physicians to liability. Gong Xiangyang, Director of the Department of Radiology at Zhejiang Provincial People's Hospital, stated that it is challenging to balance both specificity and sensitivity. Therefore, many companies prioritize sensitivity during system development, aiming to improve specificity while ensuring high sensitivity.
It should be noted that the sensitivity and specificity data reported by some companies are currently derived from specific datasets rather than clinical data. These data only demonstrate their research progress and are not suitable for comparative analysis.
Similarly, training datasets vary across companies. A larger dataset merely indicates strong relationships with hospitals and does not necessarily reflect superior system performance. Furthermore, data quality, completeness, and annotation standards differ among providers, making such data incomparable.
V. AI Issues in This Subsector
1. Definition of the optimization objective, i.e., how the problem itself is defined
2. Whether sufficient usable data can be obtained.
3. Model Interpretability
VI. Cross-Disciplinary Collaboration in “Medical Imaging AI+”
Medical imaging has become the most popular application of artificial intelligence in healthcare. A large number of AI startups have emerged in China’s medical imaging sector, and major corporations such as Tencent and JD.com have also begun to lay out their strategies, focusing on enabling machines to identify lesions and determine whether tumors are benign or malignant. However, at present, most companies rely solely on imaging data for their assessments.
VCBeat has previously interviewed a series of physicians, who stated that while machine-based lesion detection indeed helps reduce missed diagnoses and improve efficiency, determining the benign or malignant nature of tumors and identifying the specific type of cancer requires integration of clinical data, pathological findings, and even genetic sequencing. Radiological imaging alone can only identify the location and size of tumors.
In summary, there are two emerging models for collaborative R&D in medical AI: independent development and consortium-based collaboration. Unlike Alibaba or Baidu, which aim to build comprehensive platforms, these models emerge organically from actual clinical, hospital, and corporate needs, forming natural business or R&D paradigms.
“AI + Medical Imaging,” akin to the “Internet Plus” concept, currently collaborates in areas such as clinical information, genetic testing, and pathology data. However, it is poised to expand into broader domains of medical artificial intelligence in the near future. Moreover, future collaborations will not be limited to models centered solely on AI for medical imaging; instead, they may involve cross-disciplinary cooperation among various sectors of medical AI. This approach will facilitate the practical implementation of AI-powered medical imaging products, bringing them closer to real-world clinical scenarios in hospitals and enabling them to serve effectively as assistants to physicians.
The full table of contents for the “2017 Medical Big Data and Artificial Intelligence Industry Report” is as follows: