Medical Consortiums in China: Rapid Expansion, Enthusiastic Participation by Major Hospitals, Diversified Models, and Over 20 Specialized Consortia Launched – 2017 Year-End Review
In 2017, the development of medical consortiums across China could be described as flourishing everywhere. Although not a new concept, it has become a driving force for the implementation of tiered diagnosis and treatment under the backdrop of the new healthcare reform, thereby being entrusted with significant responsibilities in the new era.
This year has been remarkably dynamic. Government agencies at all levels across China have issued numerous policies, prompting hospitals of all tiers to respond actively. The number of medical consortium models has increased compared to previous years, with more than 20 types of specialized medical consortiums established.
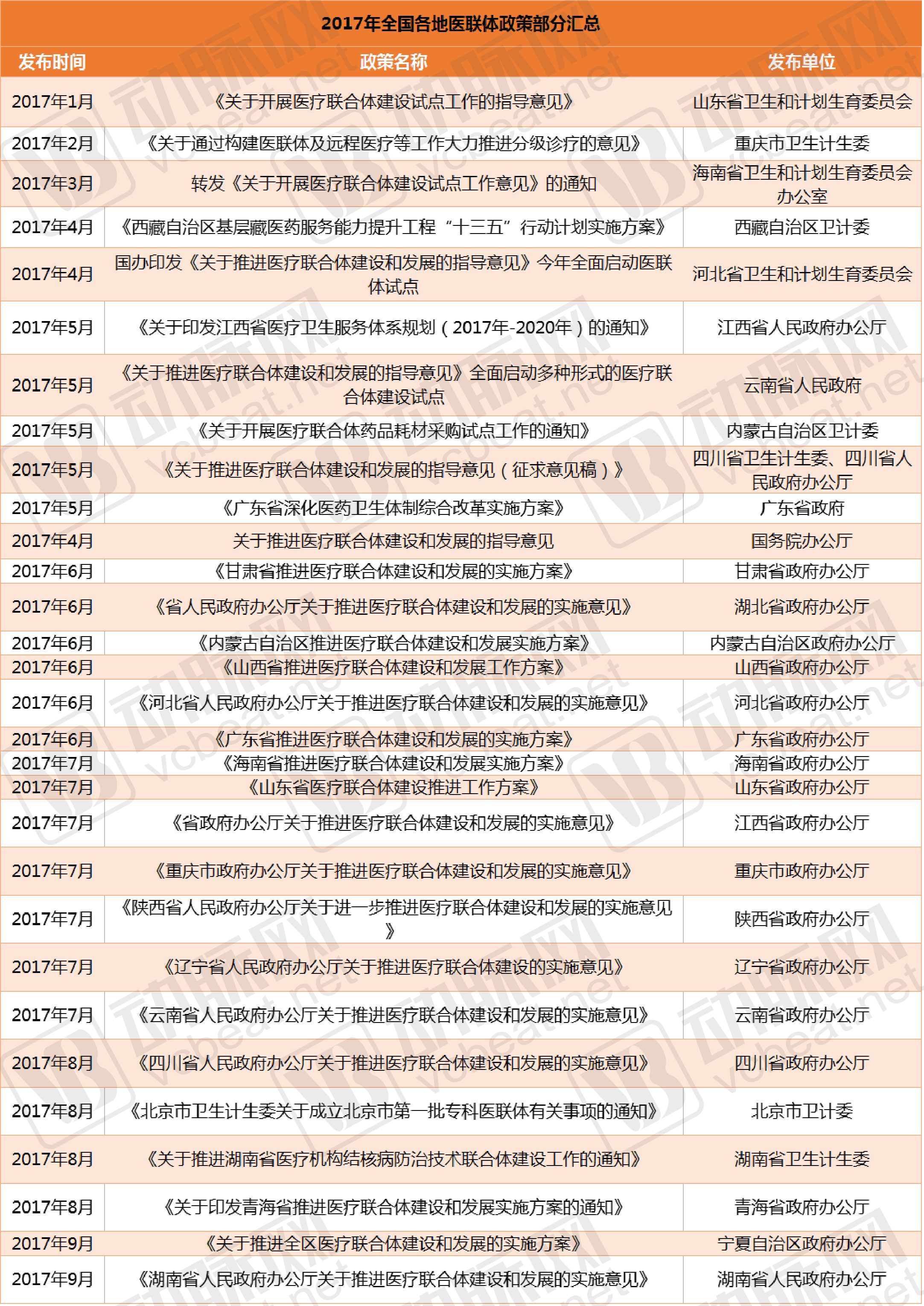
As can be seen from the list, since January 2017, policies promoting medical consortiums have been issued across China. Numerous institutions have participated in issuing these policies, including the General Office of the State Council, the National Health and Family Planning Commission, the General Office of the National Development and Reform Commission, the National Development and Reform Commission, provincial health and family planning commissions, general offices of provincial people’s governments, provincial departments of human resources and social security, provincial finance departments, municipal human resources and social security bureaus, provincial health and family planning commissions, municipal administrations of traditional Chinese medicine, municipal offices for the development of traditional Chinese medicine, municipal food and drug administrations, municipal medical insurance offices, municipal finance bureaus, municipal price bureaus, the Leading Group Office for Deepening the Reform of the Medical and Healthcare System, the Office of the Institutional Organization Committee, and municipal people’s government offices, among others.Among them, the provincial Health and Family Planning Commissions participated most frequently, followed by the General Offices of the Provincial People's Governments and the municipal Human Resources and Social Security Bureaus.
Among them, the most widely shared isOn April 23, the General Office of the State Council issued the “Guiding Opinions on Promoting the Construction and Development of Medical Consortiums.”。
The Opinion states that promoting the development of medical consortia represents a crucial step and institutional innovation in deepening healthcare reform. It facilitates the adjustment and optimization of the structural layout of medical resources, promotes the downward shift of focus and resources in healthcare services, and enhances primary care capacity. Furthermore, it enables better vertical integration of medical resources, improves the overall efficiency of the healthcare service system, and supports the effective implementation of tiered diagnosis and treatment to better meet the public’s health needs.
By the end of June 2017, all provinces (autonomous regions and municipalities) must formulate work plans to advance the development of medical consortia, specifying local targets and timelines; by the end of October, all tertiary public hospitals must initiate the establishment of medical consortia.By 2020, building on the lessons learned from pilot programs, China will comprehensively advance the development of medical consortiums and establish a relatively robust policy framework for them. All secondary public hospitals and government-run primary healthcare institutions will participate in medical consortiums.
So, after the promulgation of the medical consortium policy, what new models have emerged for medical consortia that are essentially old structures in new packaging? The details are as follows:
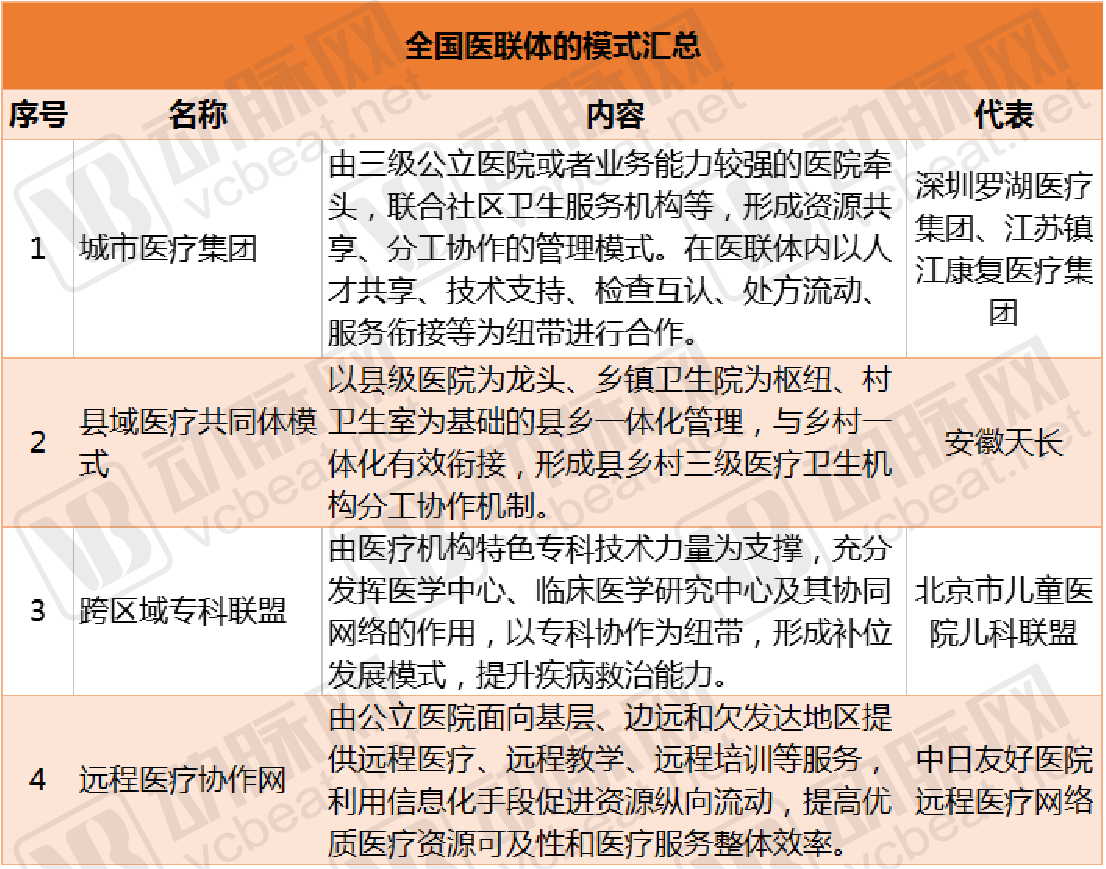
These medical consortia refer to regional healthcare alliances that integrate medical resources within a specific area. Typically, such an alliance is composed of tertiary hospitals, secondary hospitals, community health centers, and village clinics within the region, forming a collaborative network or healthcare group that functions as a community of shared interests and responsibilities. The aim is to address the difficulty patients face in accessing medical care; for instance, common ailments such as fever and colds can be managed at primary care facilities rather than overcrowding tertiary hospitals, thereby alleviating access barriers. This model has achieved the anticipated goals of satisfying the public, the government, and healthcare workers.
Based on the current composition of medical consortiums, the cooperation models among participating healthcare institutions can be categorized into two types: loose and tight. Tight medical consortiums are established on the basis of ownership and asset integration, forming a unified service delivery entity with shared financial responsibilities among member institutions. Loose medical consortiums are formed through collaboration in areas such as technology, management, information systems, and payment mechanisms, while maintaining separate asset ownership.
Currently, although medical consortia have proliferated across the board, discussions regarding which type of medical consortium is superior have never ceased.Liang Wannian, Director of the Department of Structural Reform under the National Health and Family Planning Commission, stated, “In the long run, if the division of labor among medical institutions within medical consortia is clearly defined, their roles are well-positioned, and assessment and evaluation mechanisms aligned with the medical consortium model are established, the effectiveness of tightly integrated medical consortia will be further enhanced.”
Whether medical consortiums can be successfully implemented hinges critically on the leading role played by large tertiary Grade-A hospitals. Policy directives have explicitly mandated that all public tertiary hospitals across China initiate the establishment of medical consortiums, yielding favorable outcomes.
To this end, we selected three public hospitals across China: West China Hospital of Sichuan University (hereinafter referred to as “West China Hospital”), and the First Affiliated Hospital of Chongqing Medical University (hereinafter referred to as “the First Affiliated Hospital of CQMU”),Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, let's examine how they establish medical consortiums and what results have been achieved?
To begin with, the development of medical consortiums by West China Hospital can be traced back to 2002, a time when the national government had not yet vigorously promoted such initiatives. Over the past decade-plus of building these consortiums, five distinct models have been explored. In summary, West China Hospital has established two primary types of medical consortium structures: loose and tight-knit. The representative example of the loose type is the West China Telemedicine Network Alliance Hospitals. The tight-knit type adheres to the principles of “three unchangeds, three shared resources, and three unified standards,” and includes group-based institutional alliances, led regional alliances, regional specialty alliances, and urban community alliances.
West China Remote Network Alliance Hospitals currently comprises 633 member hospitals distributed across China. The Telemedicine Center is a national-level medical education center and a regional pathology diagnostic center accredited by the National Health and Family Planning Commission. Each year, more than 500,000 person-times receive training through this platform, and over 4,000 complex cases are consulted annually. Notably, the West China telemedicine system played a significant role during the Wenchuan Earthquake.
In the development of led regional medical consortiums, West China Hospital primarily signs agreements with regional governments to deepen cooperative healthcare management. With the government as the principal party to the agreement, West China Hospital takes the lead in managing the region’s central hospital. Through both on-site and online approaches, it radiates influence to drive county-level hospitals and township health centers, thereby establishing a tiered and collaborative service system between the entire region and West China Hospital.
After more than a year of collaboration between West China Hospital and Guang’an primary care hospitals, the proportion of patients referred upward from the latter increased by 91%, while the proportion of patients transferred outside decreased by 22%;After establishing a medical consortium with Xindu, the number of inpatient visits outside the district decreased by 45.7%, and the number of outpatient visits outside the district decreased by 32.2%.
Next is the construction of the medical consortium by the First Affiliated Hospital of Chongqing Medical University. Since its inception in 2011, it has collaborated with 20 hospitals over the past six years, achieving an approximately 1:1 ratio for upward and downward patient referrals.
During the development of the medical consortium, Ren Guosheng, President of the First Affiliated Hospital of Chongqing Medical University, established a sound principle: “Even among close brothers, accounts must be kept clear.”“We regard the hospitals we support as brothers, but even between close brothers, accounts must be clearly kept. Only by making each party’s interests transparent can we achieve the objectives of a tightly integrated medical consortium.”
During this process, Ren Guosheng also established the six core components of the medical consortium: clearly defining the objectives of assistance, specifying performance indicators for such assistance, adhering to the principles of “free of charge” and “on-demand availability,” and developing a catalog of key diseases for diagnosis and treatment. To implement tiered diagnosis and treatment, it is essential to establish a catalog of key diseases for diagnosis and treatment, incorporate two-way referrals under tiered diagnosis and treatment into the performance evaluation of the medical consortium, and uphold the principle of “inviting specialists up and sending experts down.” For management and clinical staff at district and county hospitals, emphasis should be placed on the “Three Openings,” “Three Trainings,” and “Three Teams,” providing comprehensive, free, and on-demand “one-on-one” training.
As is well known, in the process of tiered diagnosis and treatment, upward referrals are often obstructed, while downward referrals lack awareness. To address this, the First Affiliated Hospital of Chongqing Medical University has established a green channel, enabling patients referred from primary care institutions to be transferred back within three to five days after surgery. However, as some primary healthcare institutions are not yet fully capable of providing adequate postoperative rehabilitation, these patients are first transferred to the hospital’s integrated medical and elderly care department, thereby freeing up limited medical resources.
Within the medical consortium led by the First Affiliated Hospital of Chongqing Medical University, when patients are referred from primary healthcare institutions to the hospital, the attending primary care physicians accompany them. These physicians participate in consultations or ward rounds alongside specialists from the First Affiliated Hospital and assist in surgical procedures under direct supervision. This hands-on mentorship enables primary care physicians to acquire the relevant clinical skills. Furthermore, this training model allows for repeated practice and mastery of the same technical procedures.
In terms of two-way referrals, from 2015 to April 2017, a total of 1,312 patients were referred upward and 1,046 patients were referred downward among the district and county hospitals within the Medical Consortium of the First Affiliated Hospital of Chongqing Medical University, resulting in an approximate upward-to-downward referral ratio of 1:1. Specifically, Dazu Hospital referred 54 patients upward and 125 patients downward.
In the construction of the medical consortium at the First Affiliated Hospital of Chongqing Medical University, it is evident that medical consortia serve as a crucial measure for promoting the vertical integration of healthcare resources. During their formation and implementation, the interests of various participating medical institutions are closely intertwined. By clarifying the strategic interactions among key stakeholders—such as the cooperative dynamics between core hospitals and member hospitals, and the competitive relationships between non-member hospitals and the medical consortium—it is possible to explore a sustainable development path for the effective operation of medical consortia. This can be achieved by improving compensation and supervision mechanisms, enhancing primary healthcare service capabilities, fostering orderly competition among medical institutions within the region, and refining corporate governance structures.
The innovative model of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, known as the “Shaw Hospital Model,” encompasses multiple dimensions, including an innovative modern hospital management system, high-quality patient care experiences, superior medical quality and safety, advanced smart healthcare platforms, and a hospital culture that is patient-centered and staff-oriented.
Public hospital reform imposes higher requirements on large public hospitals in areas such as hospital management systems, operational mechanisms, informatization, smart healthcare development, personnel and compensation systems, and collaborative development among medical institutions. In fact, during the comprehensive advancement of public hospital reform, Sir Run Run Shaw Hospital has taken a leading position in multiple aspects.
To support the development of medical service centers in core regions, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, has actively implemented the strategic plans and decisions of the Zhejiang Provincial Party Committee and Provincial Government regarding paired assistance to Xinjiang. In collaboration with multiple regional medical centers—including the First Division Hospital of the Xinjiang Production and Construction Corps, the First People's Hospital of Kashgar Prefecture, and the Second People's Hospital of Aksu Prefecture—the hospital leverages the “Sir Run Run Shaw Health Cloud Platform” to jointly create a new model of internet-based Belt and Road telemedicine collaboration.
Currently, the platform supports a range of services, including remote joint outpatient consultations, multimodal remote consultations, remote mobile ward rounds, remote imaging diagnostics, internet-based remote teaching, and mobile technical guidance. In the future, the platform will continue to deepen its service capabilities, innovate mechanisms for international medical service cooperation, expand international medical services, and actively build a comprehensive and open “Silk Road Cross-Border Medical Service Platform” to fully support the Belt and Road Initiative.
Large tertiary public hospitals are actively joining the construction of medical consortia, and numerous companies have targeted this business opportunity. According to incomplete statistics from VCBeat, there are currently 23 companies in China involved in medical consortia. These companies operate in industries such as biopharmaceuticals, medical device development, medical diagnostics, healthcare IT software development, large-scale online hospital platform development, telemedicine, and pharmaceutical distribution services.
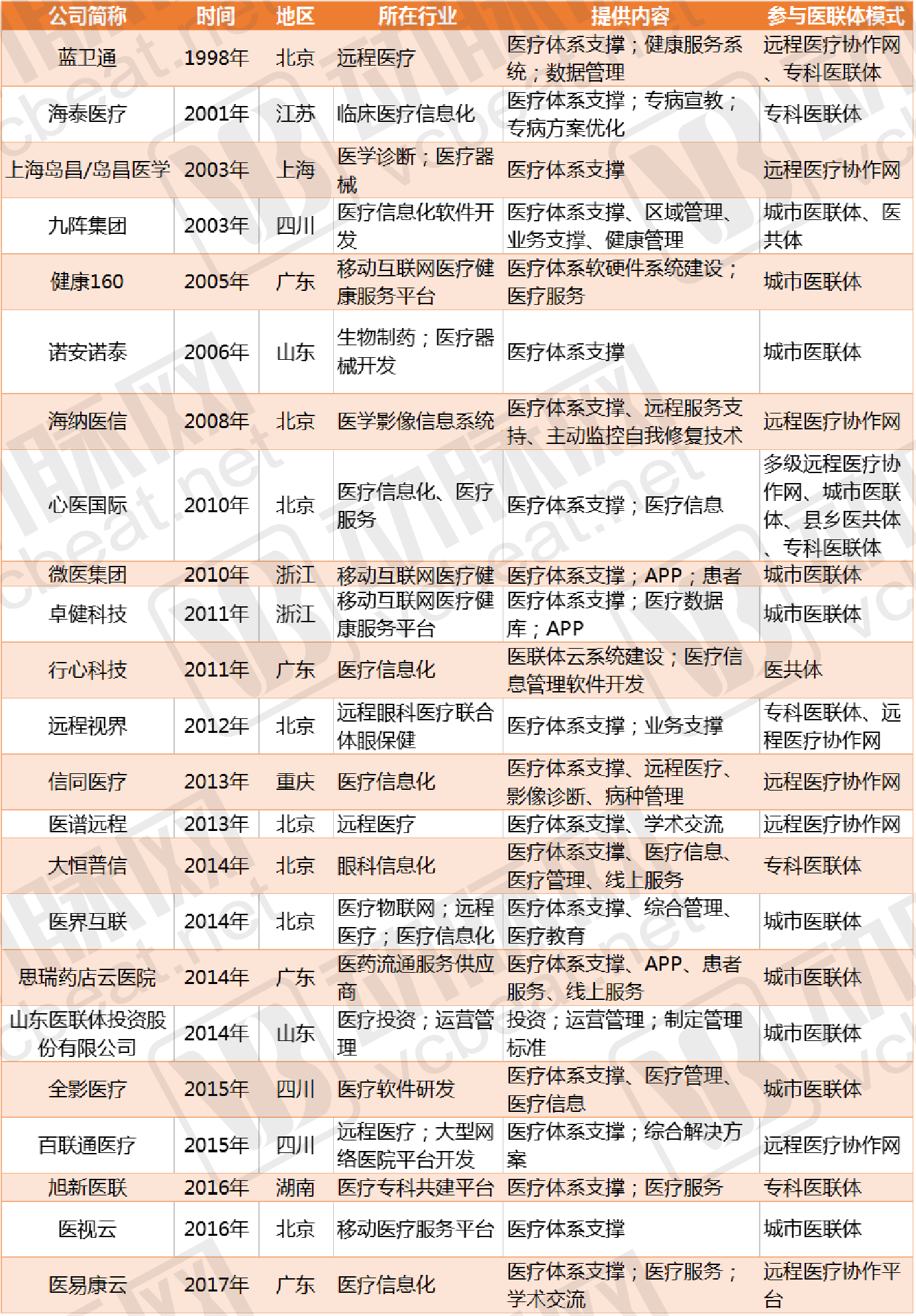
As shown in the chart, the earliest entry year for these enterprises was 1998, with a concentration of entries occurring in 2010, 2014, 2015, and 2016.
These enterprises have entered the medical consortium model by partnering with physical healthcare institutions, establishing consortia based on the needs of these entities. These include telemedicine platforms, urban medical consortia, medical communities, and specialty-specific medical consortia, aligning with the medical consortium models referenced by the State Council.
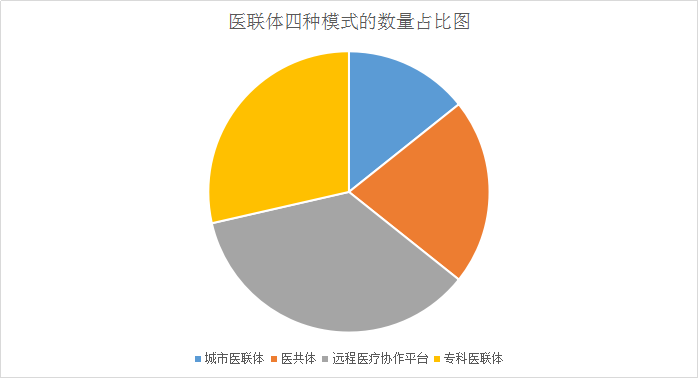
As shown in the figure above, among these enterprises involved in medical consortium models, the most common is the telemedicine collaboration platform, followed by specialized medical consortia, and then medical communities and urban medical consortia.
In the telemedicine collaboration platform, taking Xinyi International as an example, it has constructed and operated more than 20 regional and specialized medical consortium projects in Shaanxi Province, centered around major hospitals such as Shaanxi Provincial Cancer Hospital, Xi’an Honghui Hospital, Ankang Traditional Chinese Medicine Hospital, and Xijing Hospital. This has established a comprehensive and far-reaching telemedicine collaboration network, effectively alleviating the difficulties faced by residents in remote areas in accessing medical care. In addition, there are currently 50 national key poverty-stricken counties in Shaanxi Province. Xinyi International actively supports local grassroots healthcare development, implements the national health poverty alleviation strategy, and helps ensure that over 90% of these key poverty-stricken counties are covered by telemedicine diagnosis and treatment service networks.
Xinyi International has established a “five-tier integrated” telemedicine network spanning provincial, municipal, county, township, and village levels for Ankang Traditional Chinese Medicine Hospital, along with the operation of various related services. This initiative has created a multi-modal “Ankang Model” characterized by “government leadership, hospital implementation, and third-party service provision,” significantly enhancing the efficiency of the medical consortium.
By leveraging the “Ankang Xinyi International Telemedicine Platform,” the system connects with renowned domestic hospitals at the upper level and links to 75 primary healthcare institutions at the county and township levels below, extending medical service coverage down to village-level health clinics (with the Cangfang Village Health Clinic in Kazi Town, Baihe County, being the first village-level health clinic in Ankang City to adopt a remote diagnosis and treatment platform), thereby truly achieving “vertical integration to the grassroots level.”
As of September 30, 2017, the Ankang Xinyi Telemedicine Platform was operating smoothly overall. It covered 20 secondary hospitals, 43 township health centers, and 5 village clinics. The platform conducted 15 remote technical training sessions, 6 surgical observations and remote ward rounds, and trained more than 2,400 grassroots healthcare personnel. A total of 5,993 remote consultations were completed, including 634 interactive consultations and 4,943 non-interactive consultations. Among these, there were 4,514 imaging consultations, 569 electrocardiogram (ECG) consultations, and 494 clinical consultations. Consultations provided to township health centers totaled 5,102 cases, while those for secondary hospitals and above amounted to 644 cases, with 247 cases referred upward for higher-level consultation.
In the development of Medical Consortiums, Xinyi International has pioneered a comprehensive service model that empowers healthcare institutions across three dimensions—resources, technology, and services. This approach maximizes the core functions of Medical Consortiums, namely vertical integration and two-way patient referrals, thereby fully unlocking their value. Currently, its telemedicine collaboration network covers 4,300 hospitals nationwide, supports the establishment of over 120 Medical Consortium projects, and serves more than 60 national and provincial teleconsultation centers, with an annual volume of 150,000 remote diagnostic cases.
In terms of building specialized medical consortiums, WeDoctor Group has expanded into multiple areas, including pediatric, otolaryngology, traditional Chinese medicine (TCM), and reproductive medicine consortiums. The specific details are shown in the figure below:

As pointed out by the State Council’s new policy on medical consortiums, medical consortiums should be transformed into communities of service, responsibility, interest, and management. Therefore, the core of promoting the construction and development of medical consortiums lies in “integration.”
WeDoctor breaks down “integration” into five actionable pillars: data integration, capability integration, service integration, payment integration, and supply chain integration.
Data connectivity refers to the continuous recording and information sharing of electronic health records (EHRs) and electronic medical records (EMRs), enabling interoperability of diagnostic and treatment information within medical consortiums. WeDoctor has spent nearly seven years deploying over 1,700 front-end servers across China, achieving varying degrees of data interconnectivity with more than 2,400 hospitals and accumulating extensive experience in data integration across heterogeneous systems. WeDoctor’s cloud-based EMR system helps primary healthcare institutions rapidly establish EHRs and EMRs.
Capability Linkage refers to the sharing and downward dissemination of expertise from tertiary medical institutions and specialists to grassroots levels through various forms, including remote consultations, two-way referrals, remote teaching, remote training, joint development of specialized departments, clinical preceptorship, operational guidance, teaching rounds, and research and project collaboration. This approach facilitates the vertical integration of high-quality medical resources within Medical Consortiums. It also enables the sharing of capabilities such as medical imaging and laboratory testing within the Medical Consortium.
Service Linkage refers to the application of internet capabilities to provide patients with continuous diagnosis and treatment services, enabling continuous follow-up, chronic disease management, health education, and family doctor contracting services. This facilitates a shift from a medical care-centered model to a health-centered model.
Payment Consortium refers to the exploration of pooled health insurance payments within medical consortia, the introduction of commercial insurance payments, and the formation of a multi-tiered healthcare payment system.
The supply chain alliance refers to the establishment of a unified platform for drug bidding, procurement, and management within a medical consortium. It aims to reduce procurement costs through secondary price negotiations and to create mechanisms for prescription circulation, drug sharing, and distribution within the consortium.
It is evident that public demand, policy support, and technological advancements are gradually converging to form a synergistic force. Through innovation and the promotion of medical consortium development, these factors are better facilitating the implementation of tiered diagnosis and treatment.
WeDoctor’s Medical Consortium System comprises eight subsystems: remote diagnosis and treatment, remote consultation, remote referral, remote training, cloud-based electronic medical records (EMR), cloud pharmacy, cloud-based laboratory and imaging services, and payment and settlement. The system features hardware and software solutions refined through large-scale operations, referral channels connecting more than 700 major Grade-A tertiary hospitals across China, and consultation resources from over 7,300 expert teams spanning 28 medical specialties. After nearly seven years of accumulation, WeDoctor has amassed more than 172 million real-name authenticated patients and established medical and operational teams in 32 provinces and municipalities. It is now scaling the output of its three core capabilities—system infrastructure, user traffic, and operational expertise—to assist major public hospitals in establishing medical consortia.
According to public data, a wide variety of specialized medical consortia have emerged in China. A total of 27 types of specialized medical consortia have been established across the country, covering specialties such as pediatrics, otolaryngology, rheumatology, gynecology, maternal and child health, hepatology, orthopedics, respiratory medicine, and laboratory medicine. Among these, pediatrics has the largest number of departments, followed by mental health, stomatology, and pain management. As shown in the figure:

Specialized Medical Consortiums are one of the four models of medical consortiums. Most are cross-regional alliances that place greater emphasis on improving medical technical expertise and talent development within specific specialties, thereby providing homogeneous services and standardized diagnosis and treatment protocols across the consortium. Core hospitals and member hospitals can collaborate professionally to categorize diseases and unify diagnostic and therapeutic standards. These consortia are formed through specialized collaboration, anchored by the distinctive specialty of one medical institution and integrating similar specialty capabilities from other institutions. This approach establishes several regional centers of excellence for specific specialties, enhances the capacity to manage and treat major specialized diseases, and fosters a complementary development model.
As specialized medical alliances have effectively bridged the critical nodes of tiered diagnosis and treatment, numerous such alliances have emerged across China, increasingly becoming a prevailing trend. During their development, however, differences in traditions, systems, and management models among medical institutions at various levels have led to unique characteristics across departments, leaving no fixed or mature model to follow.
Furthermore, medical institutions at all levels have their own vested interests. If inter-institutional relationships are not effectively coordinated, it will be difficult to establish specialized medical consortia; even if they are established under duress, they will struggle to fulfill the intended role of “managing minor illnesses in the community, referring serious cases to hospitals, and returning patients to the community for rehabilitation.”
The development of specialized medical consortia should adopt a point-to-area approach, identifying precise breakthrough points to achieve initial success that drives broader progress. This ensures that all member institutions, healthcare professionals, and patients within the consortium benefit, thereby effectively implementing tiered diagnosis and treatment.
Thus, it is evident that although the development of medical consortia in 2017 achieved a series of accomplishments, the mission remains incomplete, and healthcare institutions at all levels must continue their efforts.
Next year, the development of medical consortia may face greater challenges, primarily in the following three areas:
First, supply-side structural reform has brought new challenges to the reform of public hospitals. The reform of urban public hospitals aims to resolve contradictions in their systems and mechanisms; the establishment of a tiered diagnosis and treatment system is intended to correct distortions in resource allocation.
Second, the expansion of the connotation and extension of social service demands poses challenges to such hospitals;
Third, technological advancements have brought new challenges and opportunities to the transformation of healthcare service models;
Fourth, the implementation of policies such as zero markup on drugs and multi-site practice for physicians has created a forcing mechanism for the operation and development of public hospitals. If they do not take the initiative to reform, the development pathways available to public hospitals may become increasingly narrow in the future.
Faced with numerous challenges, tertiary hospitals must first clarify their positioning and determine which conditions they should accept for treatment and which they should not.
Next, strive to enhance the capability to manage complex cases referred from other hospitals. When patients who cannot be treated elsewhere are transferred to your facility for care, you must be fully equipped to handle them. This requires advanced clinical expertise and innovation, enabling you to perform interventions that others cannot.
Although the tiered diagnosis and treatment system has diverted patients with common and frequently occurring diseases, those who can achieve the above two points may still not lack patients.
If you are following “Medical Consortium Development,” you are welcome to register for the event to be held in Beijing from December 15–17.“2017 Future MedicineTop 100 in Healthcare"Forum, we will dedicate an entire day to the "Hospital Innovation Parallel Forum”, inviting four innovative hospital deans and multiple enterprise founders to discuss two key themes: “Medical Consortium Development” and “How to Improve Hospital Operational Efficiency.” Long-press the image below to scan the QR code and register.
