AI-Powered Chronic Disease Management Platform Aims to Transform Medical Consortiums: AYISHENG Health Files for IPO
“Caring for the lifelong health of hundreds of millions” is a phrase that Jin Xin, founder of Aiyisheng Health (hereinafter referred to as “Aiyisheng”), often repeats; indeed, the company derives its name from this motto. In his view, Aiyisheng has always been a technology-driven enterprise. His entrepreneurial strategy focused on entering the market segment with the lowest penetration of internet applications yet the greatest potential. From a humanitarian perspective, he believes entrepreneurship should serve as a force for good, benefiting both the nation and its people. Thus, leveraging technology to transform chronic disease management has remained Jin Xin’s unwavering choice from the outset.
At the Hospital Innovation Parallel Forum of the “2017 Top 100 Future Healthcare Companies” forum, Jin Xin delivered a keynote speech titled “Empowering Medical Consortium Development with AI-Driven Chronic Disease Management,” elaborating on the logic behind Aiyisheng’s products in facilitating medical consortium construction and their application scenarios. To further explore the implementation status of Aiyisheng’s National Guideline-based AI Chronic Disease Management System (hereinafter referred to as the “GDS System”), after the conference,VCBeat (WeChat: vcbeat)"Reporters conducted an exclusive interview with Jin Xin."

Jin Xin, Founder of Aiyisheng Health
The Challenges of Chronic Disease Management Lie in Payment Issues and Decentralized Primary Care Management
According to data released by the World Health Organization in 2016, one in ten people in China has diabetes. Furthermore, at the Symposium on Action Plans for the Prevention and Control of Cardiovascular Diseases in China, held in Beijing in May 2016, experts pointed out that deaths attributable to four major chronic diseases—cardiovascular disease, cancer, diabetes, and respiratory diseases—accounted for 86.6% of all deaths, indicating a very severe situation in the prevention and control of chronic diseases.
China was the first country to launch a national-level plan for chronic disease prevention and control. As early as May 2012, the "China National Plan for Chronic Disease Prevention and Control (2012–2015)" was introduced, involving 15 national ministries and commissions. In January 2017, the General Office of the State Council issued the "Medium- and Long-Term Plan for Chronic Disease Prevention and Control in China (2017–2025)." This marked the first time that a chronic disease prevention and control plan was issued under the name of the State Council. The plan explicitly set forth core objectives to reduce premature mortality rates from cardiovascular and cerebrovascular diseases, cancer, chronic respiratory diseases, and diabetes among individuals aged 30–70 by 10% by 2020 and by 20% by 2025, compared with 2015 levels, and proposed 16 specific operational indicators. The elevation of chronic disease prevention and control to the national level further underscores the substantial demand for chronic disease management in China.
Established in February 2014, Aiyisheng Health has dedicated a decade to core technology R&D, focusing on the field of intelligent healthcare. The company translates clinical practice guidelines into translational medical research to develop clinical decision support tools, providing an AI-driven chronic disease management system aligned with national guidelines. The development of these tools for chronic diseases addresses the significant challenges prevalent in this sector.Jin Xin believes that the challenges of chronic disease management lie in two aspects:
1. Payment issues.China’s medical insurance system has long prioritized coverage for major illnesses and inpatient care. This model proves inadequate in addressing the explosive growth of chronic diseases, leaving it capable only of passive response. Under the current system, reimbursement rates for inpatient services are high, while those for outpatient services are low or even nonexistent. Furthermore, expenses related to chronic disease management and health prevention fall outside the scope of medical insurance reimbursement.
In such circumstances, two extreme phenomena emerge: either minor ailments are overtreated with hospitalization as the primary goal to secure higher reimbursement rates, thereby wasting bed resources; or minor conditions are left untreated and unprevented, with hospitalization sought only after problems arise. Both scenarios result in substantial depletion of medical insurance funds.
Jin Xin believes that it is crucial to integrate health insurance into the overall chronic disease management system, thereby supporting corresponding family doctor contract services, facilitating tiered diagnosis and treatment and two-way referrals within medical consortia, and ultimately underpinning the entire chronic disease ecosystem.
Second, chronic disease management must be carried out at the primary care level.In 2015, the State Council issued the “Guiding Opinions on Promoting the Construction of a Tiered Diagnosis and Treatment System,” which proposed to focus on enhancing the capacity of primary healthcare services, with tiered diagnosis and treatment for common diseases, frequently occurring diseases, and chronic diseases as the breakthrough point. In 2015, priority was given to pilot programs for the tiered diagnosis and treatment of hypertension and diabetes. A tiered diagnosis and treatment model featuring initial consultation at primary care institutions, two-way referral, separate management of acute and chronic conditions, and coordination between upper- and lower-level medical institutions has gradually taken shape, thereby establishing a tiered diagnosis and treatment system fundamentally aligned with China’s national conditions.
From a policy perspective, this is undoubtedly the correct direction. Jin Xin believes, “Chronic disease management must essentially be carried out at the primary care level. Tertiary Grade A hospitals cannot effectively manage patients with chronic diseases; physicians are already overloaded, struggling to see each outpatient within just three to five minutes. Thus, our medical resources are limited.” Consequently, the heavy responsibility for chronic disease management falls on primary care institutions. Although China has 20,000 community health service centers, the reality at the grassroots level is far from optimistic, with persistent problems such as shortages of medical staff and medications, difficulties in data collection, talent deficits, and insufficient motivation among primary care providers.How community health institutions utilize their resources is crucial.
Chronic Disease Ecosystem Requires Technological Innovation
"In every aspect of chronic disease management, given the constraints of limited resources, technology serves as the primary productive force for an innovative system."Citing Professor Cai Jiangnan’s concept of “disruptive technology,” Jin Xin believes that technological innovation, particularly artificial intelligence (AI), is critical to chronic disease management. “In discussions with experts from Beijing Fuwai Hospital and Beijing Anzhen Hospital, we reached a consensus that without AI, China cannot achieve its goals in chronic disease management. Strengthening primary care requires robust support from the healthcare ecosystem.”
Therefore, for the past decade, Aiyisheng Health has focused on the fields of smart healthcare and chronic disease management, integrating artificial intelligence technology with clinical medicine. It provides the GDS (Guideline-based AI Chronic Disease Management System) aligned with national guidelines, and is committed to building an intelligent medical engine for the chronic disease healthcare ecosystem, supporting chronic disease prevention and control for the entire population as well as refined chronic disease management for key populations.
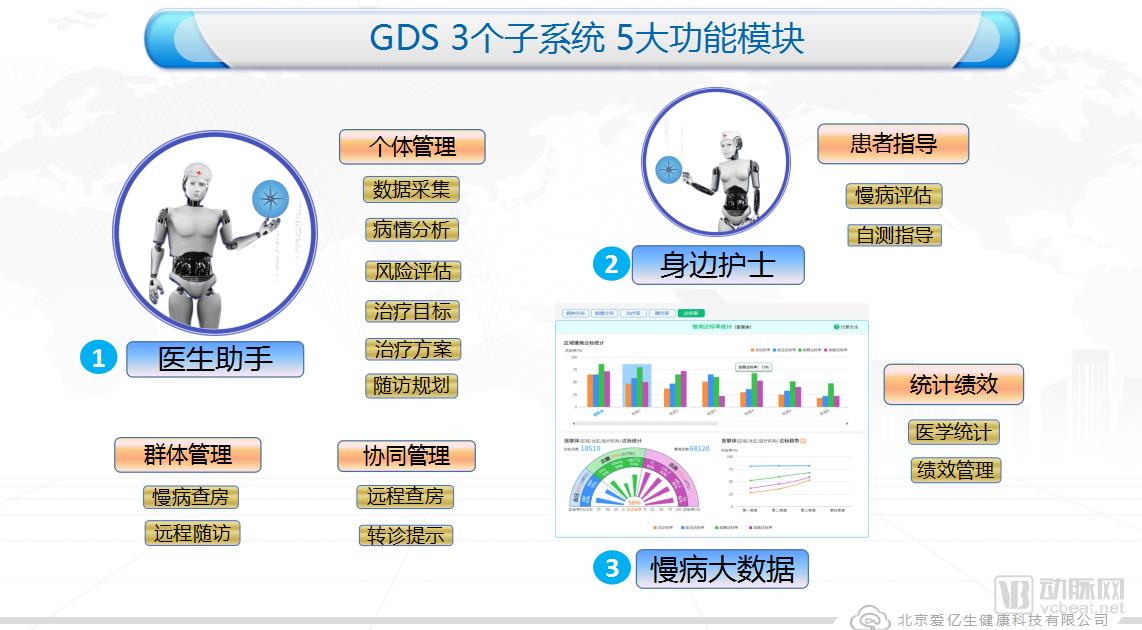
The GDS National Guideline AI-Based Chronic Disease Management System currently covers seven major conditions: hypertension, diabetes, dyslipidemia, coronary heart disease, cerebrovascular disease, gout, and hyperhomocysteinemia. It comprises three subsystems—Physician Assistant, Personal Nurse, and Chronic Disease Big Data—as well as five functional modules: individual management, population management, collaborative management, patient guidance, and medical management.
In the three major application scenarios of community hospitals, regional medical consortia, and urban chronic disease ecosystems, the GDS system assists physicians by acting as a clinical decision support tool and providing patient guidance; serves as a virtual nurse for patients; supports hospital administrators, health commissions, and social security agencies by offering a healthcare management platform; and builds an integrated ecosystem for healthcare services, health insurance, and pharmaceuticals (“Three-Medical Linkage”), while providing operational platforms for commercial insurance and pharmaceutical industries. The GDS system supports the management of patient panels under contract with community family doctors, and collaborates with specialists, general practitioners, and health managers to play a pivotal role in the tiered diagnosis and treatment medical consortium.
In Jin Xin’s view, the GDS system functions like an engine, driving all aspects of the chronic disease ecosystem—including physicians, patients, hospital administrators, the National Health and Family Planning Commission, social insurance, commercial insurance, and pharmaceutical resources—to form a community of shared interests centered on therapeutic efficacy and health outcomes.
Background of the Implementation of the GDS System in the National-Level Healthcare Reform Demonstration Zone
Three key terms in China’s healthcare reform include: family doctor contracting, tiered diagnosis and treatment, and the coordinated development of medical care, health insurance, and pharmaceuticals. Jin Xin is thoroughly familiar with the situations of Aiyisheng’s two most representative partners—the Beijing Fangzhuang Community Health Service Center and the Shenzhen Luohu Hospital Group. The former is a model for primary healthcare in China, while the latter represents the most typical example of medical consortium development in the country. He believes that the successful implementation of the GDS system is closely linked to the profound healthcare reform backgrounds of these two national-level demonstration projects.
Beijing Fangzhuang Community Health Service Center
Beijing Fangzhuang Community Health Service Center is the most advanced community medical institution in China, particularly renowned for its innovative practices. As early as early 2014, Beijing Aiyisheng Healthy Science And Technology Co., Ltd. established a close partnership with Fangzhuang, successfully launching its first pilot project there. Currently, the center serves a population of 100,000 within its jurisdiction. In the broader context of tiered diagnosis and treatment and the downward allocation of healthcare resources, grassroots community health service centers are no longer limited to providing outpatient services akin to those of hospitals; instead, they have begun offering more comprehensive health management services.
Within a 2-kilometer radius of the Fangzhuang Community Health Service Center, there are two tertiary Grade A hospitals: Tiantan Hospital and Dongfang Hospital. Consequently, a medical consortium model known as the “Fangzhuang–Tiantan Hospital” partnership has been established in this area.At the overall level, the demand for community health service centers is to provide “family doctor-style” services and guide initial consultations at the community level.
According to Jin Xin, the GDS system performed three key functions within the “Fangzhuang–Tiantan Hospital” medical consortium model: first, it provided an appointment-based consultation system; second, it delivered refined health management services to the local population, including chronic disease assessment, intervention plans, scheduled reminders, health monitoring, and follow-up appointments; and third, it facilitated two-way referrals between the Fangzhuang Community Health Service Center and Tiantan Hospital as well as Dongfang Hospital.
Shenzhen Luohu Hospital Group
Shenzhen Luohu Hospital Group established a tightly integrated medical consortium with a single legal entity in August 2015, becoming a pioneer in promoting the practice of tiered diagnosis and treatment. Its five district-affiliated hospitals and 23 directly affiliated community health centers cover the entire population of 1 million in Luohu District, Shenzhen. As part of the healthcare reform objectives, every community health center under Luohu Hospital displays a banner at its entrance, which reads:“Fewer illnesses, fewer hospitalizations, lower burden, better care”, Jin Xin believes: “These 12 characters have become a shared goal for collective efforts, while the true driver of Luohu’s healthcare reform is the reform of the medical insurance fund.”
The healthcare fund reform of Luohu Hospital Group can be summarized in eight characters: "global budget management, retention of surplus."In other words, refine the total amount and control the indicators.Taking the total medical expenses for 2017 (S) as an example, the state calculates the total amount paid from the basic medical insurance critical illness pooling fund and the local supplementary medical insurance fund for hospitalization among the contracted and insured population in Luohu District in 2015 (M), while also incorporating the growth rate of Shenzhen’s medical insurance fund expenditures in 2016 (r), to determine the overall funding allocated by the state to Luohu District in 2017. The calculation formula is as follows:
S=M x (1+r)
Specifically, three conditions must be met: First, the healthcare group shall not restrict contracted residents’ choice of medical providers. Second, the group shall not participate in health insurance cost containment for contracted residents seeking care at medical institutions outside the group; the health insurance portion of payments for such out-of-group care shall be deducted from the global health insurance fund budget. Third, health insurance expenditures for care received outside the Luohu Hospital Group shall be paid from the group’s global budget.
Jin Xin stated, “This reform of the medical insurance fund is essentially leveraging medical insurance to compel hospitals to strengthen primary care facilities, decentralize resources, and retain patients within the community.”As early as 2015, Aiyisheng began collaborating with Shenzhen Luohu Hospital to implement its GDS artificial intelligence chronic disease management system. As a centerpiece of the healthcare reforms undertaken by the Luohu Hospital Group, chronic disease management has been significantly enhanced by the GDS system, which assists general practitioners in greatly improving their efficiency and plays a vital role in the development of the medical consortium.
Fangzhuang Community Health Service Center enables residents to receive their initial consultations within the community through family doctor-style contracted services, while Luohu aims to retain residents in the community by implementing a series of measures to decentralize healthcare resources. For these two pioneers of healthcare reform, Fangzhuang and Luohu, a major focus and challenge lies in effectively leveraging their roles at the community and primary care levels to align with the trend of tiered diagnosis and treatment.
How Aiyisheng “Empowers” Medical Consortia
Jin Xin believes that the service capability of primary care general practitioners is a threshold that must be crossed to ensure effective chronic disease management at the grassroots level. Aiyisheng’s approach to supporting the construction of medical consortia focuses on three key aspects:
First, residents must be able to "stay" in their communities.The GDS system supports family doctor contract services by integrating “reputation” and “branding,” thereby enhancing residents’ sense of gain and healthcare experience. It provides community health centers and other institutions with professional, standardized services guided by national guidelines, and delivers refined chronic disease management for residents within the jurisdiction, including the formulation of annual follow-up plans and scheduling of follow-up visits.
Second, community hospitals must be able to “handle the load.”Provide professional support to community hospitals through physician assistants, quantitative chronic disease management technologies, and chronic disease assessment reports, thereby building an integrated ecosystem for community-based home rehabilitation and comprehensive chronic disease management;
Third, ensuring high-quality medical care.Internal collaboration within the Medical Consortium provides a seamless referral platform and chronic disease ward-round technology, enabling specialists and general practitioners to conduct remote chronic disease rounds. It offers intelligent follow-up management, allowing patients to receive hospital-grade, premium chronic disease medical services through follow-ups or in home-care settings.
Fourth, the introduction of an AI-powered chronic disease management system based on national guidelines to provide systematic clinical medical support.The GDS system, which integrates 18 national clinical practice guidelines for chronic diseases, covers seven major conditions: hypertension, diabetes, dyslipidemia, coronary heart disease, cerebrovascular disease, gout, and hyperhomocysteinemia. By leveraging artificial intelligence technology, it translates national guidelines into clinical guidance, creating a powerful engine for chronic disease management.

Ecological Positioning of the National Guidelines for AI-Based Chronic Disease Management (GDS)
Jin Xin views the GDS system as a medical engine, vividly describing it as the “most powerful brain” for chronic disease management.“This system can be envisioned as a virtual robotic physician, known as the ‘Physician Assistant,’ which provides support to primary care physicians. The second component is the ‘Personal Nurse,’ which safeguards patients via the cloud and delivers on-demand professional guidance through patient-facing mobile apps or WeChat official accounts. It generates comprehensive chronic disease assessment reports to assist physicians in evaluating patients’ health status. Thirdly, the system leverages big data on chronic diseases to provide hospital administrators and government agencies with a platform for medical statistics and performance management. This includes data on the distribution and trends of chronic diseases and conditions within the jurisdiction, treatment and follow-up tracking, and statistics on guideline-based individualized attainment rates for blood pressure, blood lipids, and blood glucose. By integrating population-level big data with precise, individualized detailed indicators, the system enhances the effectiveness of contracted services provided by family physician teams and ensures that government policies on large-scale chronic disease management are supported by clinical data, thereby constructing an ecological closed loop for chronic disease management.”
Connecting primary care facilities, hospitals, government agencies, insurance providers, and pharmaceutical companies, the GDS system currently covers 100 medical institutions and manages 1 million patients with chronic diseases.
In Jin Xin’s eyes,“Empowerment” is a very important word.He believes that serving the 300 to 400 million people with chronic diseases cannot rely on a few doctors alone, but rather requires a collective effort. Therefore, the overall service capacity of family doctors is crucial, while the current competency level of primary care physicians remains uneven. Thus, the empowerment provided by Aiyisheng lies inBy leveraging information technology, the service content and framework for chronic disease management and family doctor services are standardized.“Use intelligent tools to guide primary care physicians on what to do at each step, define your service offerings and target objectives, establish standardized and professionalized workflows, and enhance overall service capabilities.”
Currently, the implementation scenarios of Aiyisheng have begun to expand from primary care settings to medical consortia. Jin Xin believes that, given the prerequisite that all major hospitals must participate in medical consortia, these consortia will become important operational units for chronic disease management.
Under the strategic positioning of “primary care + medical insurance,” Aiyisheng has gradually begun to move toward developing an urban healthcare ecosystem. In 2017, Aiyisheng partnered with Ping An Insurance to launch China’s first HMO/PBM pilot in a major coastal city in a northern province. The initiative aims to collaborate with commercial insurers and pharmaceutical companies to support government health commissions and social security agencies in building an urban chronic disease management ecosystem.
Jin Xin told reporters that, mirroring the developmental trajectories of Europe and North America, the incidence of chronic diseases peaked during the post-World War II economic recovery. As chronic disease management became more widespread, prevention and control outcomes continuously improved. Similarly, China’s chronic disease management is expected to reach a turning point only after its economic development and public health awareness have attained certain levels. Therefore, Aiyisheng is currently focusing its practices on coastal developed cities and first-tier cities, where greater emphasis is placed on chronic disease management and patient compliance is relatively high. Meanwhile, the company has also initiated explorations into chronic disease management in central and western regions as well as county-level areas in inland provinces, aiming to rapidly establish demonstrative models tailored to different geographic regions and levels of economic development, thereby accelerating their promotion and replication.
Further refining the tools and methodologies for chronic disease management is an ongoing process. In the closing remarks of the interview, Jin Xin told reporters that Aiyisheng is currently focused solely on the exploration and R&D of smart healthcare solutions for chronic disease management, with no immediate plans to expand into other fields. The path to effective chronic disease management is fraught with challenges, and companies operating in this space must recognize the significant responsibilities and long journey ahead. As the burden of chronic disease prevention and control increasingly shifts to primary care settings with relatively limited resources, “forcing change through pressure” may not be the ideal approach, but it remains the most direct and effective method within the current healthcare ecosystem. Ultimately, “strengthening primary care” must hinge on technological innovation and service transformation. The concept of “empowerment” should deliver value at every stage, helping to build a clearer and more effective ecosystem for chronic disease management.