Prospectus of the Report on the Development Status of China's Primary Healthcare Industry: 4% of Township Health Centers Generate 52% of Medical Revenue
Preface
The government introduced the tiered diagnosis and treatment system and the medical consortium system to promote the downward flow of high-quality medical resources, achieve resource sharing, and address the lagging development of primary healthcare. Primary healthcare has gained new momentum and entered a new stage of development. However, disparities in regional economic development and between urban and rural areas, coupled with an inherent shortage of high-quality medical resources in rural primary care, have exacerbated imbalances in the development of primary healthcare. To achieve the healthcare reform goal of equalizing access to basic medical services, it is essential to redistribute medical resources and increase support for the primary care level.
Primary healthcare accounts for as much as 95% of China’s entire medical and health system, encompassing community health service centers (and stations), township (and sub-district) health centers, village clinics, and outpatient departments. With the gradual implementation of healthcare reform policies, there has been significant improvement in the scale, workforce size, and service capacity of primary healthcare in China. However, compared with hospitals of higher tiers, primary healthcare institutions still face deficiencies in bed supply and equipment sophistication, and the imbalance between urban and rural development remains a prominent challenge.
Indicator Explanation:
① Primary healthcare institutions: mainly including four types of institutions, namely community health service centers (stations), township (sub-district) health centers, village clinics, and outpatient departments.
② Public and private institutions: The former refers to medical and health institutions with state-owned or collective economic ownership; the latter refers to medical and health institutions with economic ownership other than state-owned or collective, including those operated through joint ventures, shareholding cooperatives, private enterprises, and investments from Hong Kong, Macao, Taiwan, and foreign countries.
③ Urban and Rural Scope: Urban areas include districts of municipalities directly under the Central Government, districts of prefecture-level cities, and county-level districts; rural areas include townships and administrative villages.
④ Research Methodology and Data Sources: This report primarily employs a literature review approach. By systematically analyzing official data released by the National Health and Family Planning Commission—including the China Health and Family Planning Statistical Yearbook and the Statistical Bulletin on the Development of Health and Family Planning in China—it provides a comprehensive analysis of the current state of grassroots healthcare development.。
Healthcare Institutions: Numerical Dominance Overshadows Pronounced Developmental Imbalances

Total Volume Rises, Growth Rate Slows:Between 2011 and 2016, the number of primary healthcare institutions in China showed an overall upward trend, albeit with a relatively slow growth rate. Notably, in 2012, there was a significant decline in the number of these institutions, primarily driven by a reduction in village clinics. As urbanization accelerated, the rural population decreased year by year, leading to a corresponding decline in the number of village clinics.

Overwhelming Numerical Advantage:Primary healthcare institutions account for approximately 95% of the entire medical and health institution system, playing a significant role in the development of China’s healthcare sector. In contrast, hospitals, which contribute 78% of the total revenue of medical institutions in China, constitute only 3% of the total number of such institutions.
Proportion by quantity has decreased:The proportion of primary healthcare institutions decreased by 2 percentage points. During the same period, the proportions of hospitals and specialized public health institutions increased by 0.7 and 1.3 percentage points, respectively. As a key pillar of China’s healthcare service system, hospital construction has maintained steady growth.
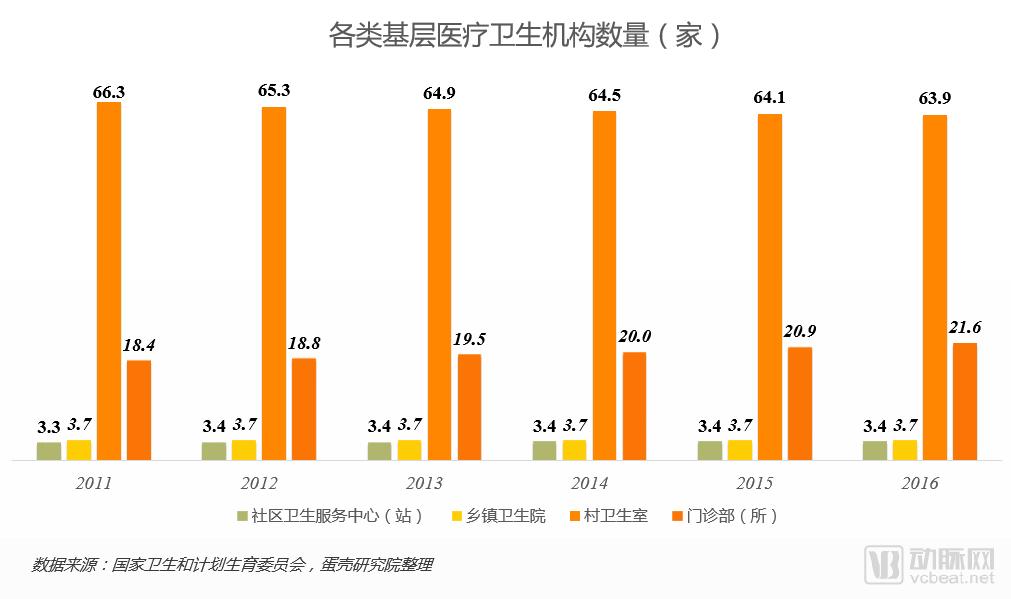
Leading Number of Village Clinics:Among all types of primary healthcare institutions in China, village clinics account for 70%, far surpassing other institutions and providing a guarantee for rural medical services.
Outpatient Clinics Show Strong Growth Momentum:The number of outpatient departments (clinics) has risen year by year, with an overall increase of 17% from 2011 to 2016, thanks to the relaxation of policy requirements for establishing clinics.
The number of township health centers remains stable:In recent years, the number of township health centers has remained stable at approximately 37,000, primarily because China’s township administrative divisions have remained unchanged.
Insufficient Development of Community Health Service Centers (Stations):
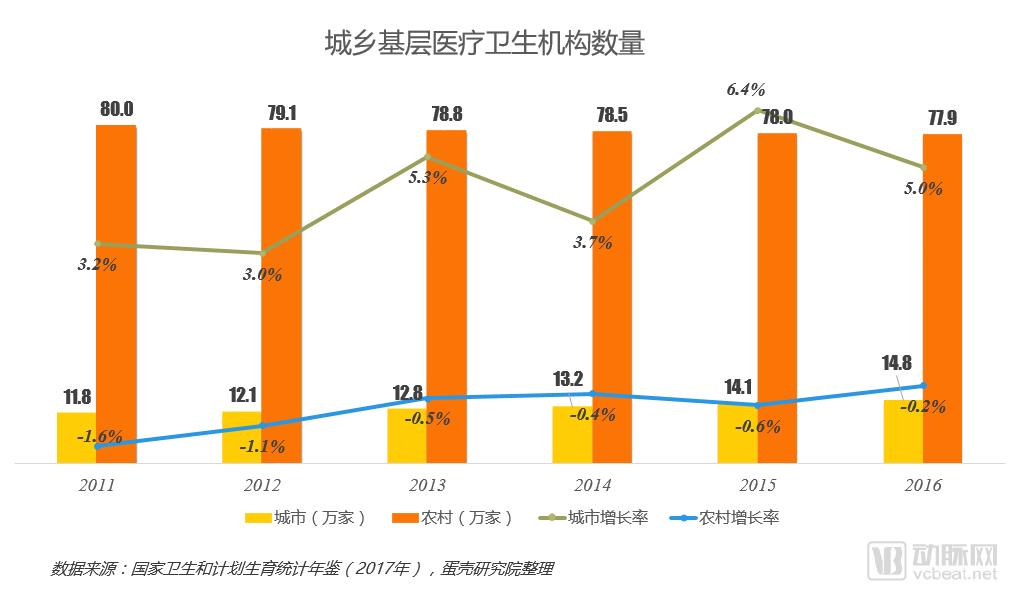
The Number of Rural Institutions Far Exceeds That of Urban Areas:This is mainly because the rural population is large and relatively dispersed, and village clinics are numerous; therefore, more medical institutions are required to achieve comprehensive coverage.
Divergence in Growth of Urban and Rural Primary Healthcare Institutions:The number of primary healthcare institutions in rural areas continues to decline, while that in urban areas keeps increasing. Urbanization has accelerated the migration of the rural population to cities, leading to a continuous expansion of urban medical demand and driving the growth in the number of urban primary healthcare institutions.
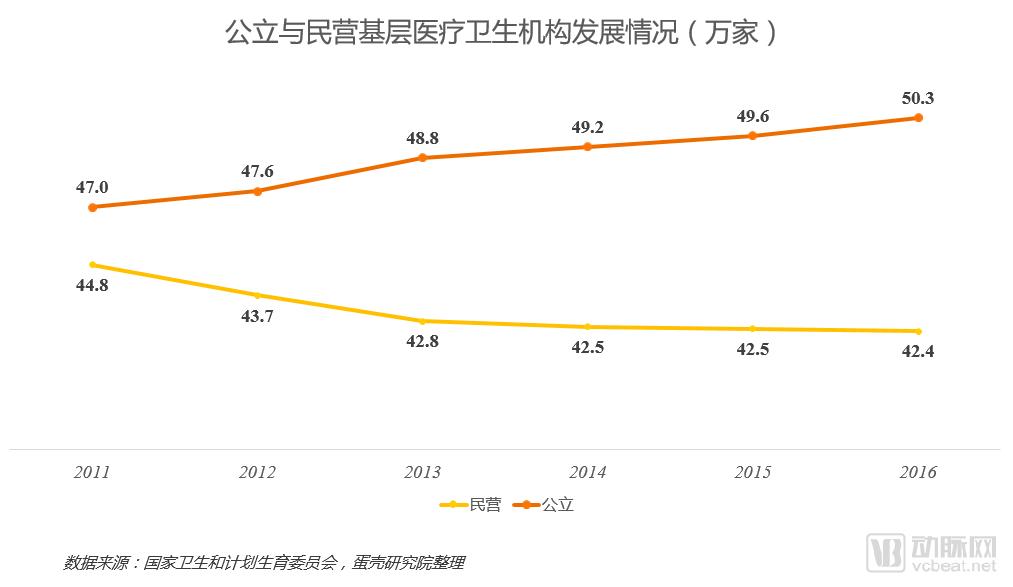
Public Sector as the Mainstay, Private Sector as the Supplement:Public primary healthcare institutions outnumber private ones, with the number of public facilities continuing to rise while the number of private facilities continues to decline. This is primarily because primary healthcare institutions (particularly in rural areas) have limited profit margins, resulting in low enthusiasm for participation by private capital.
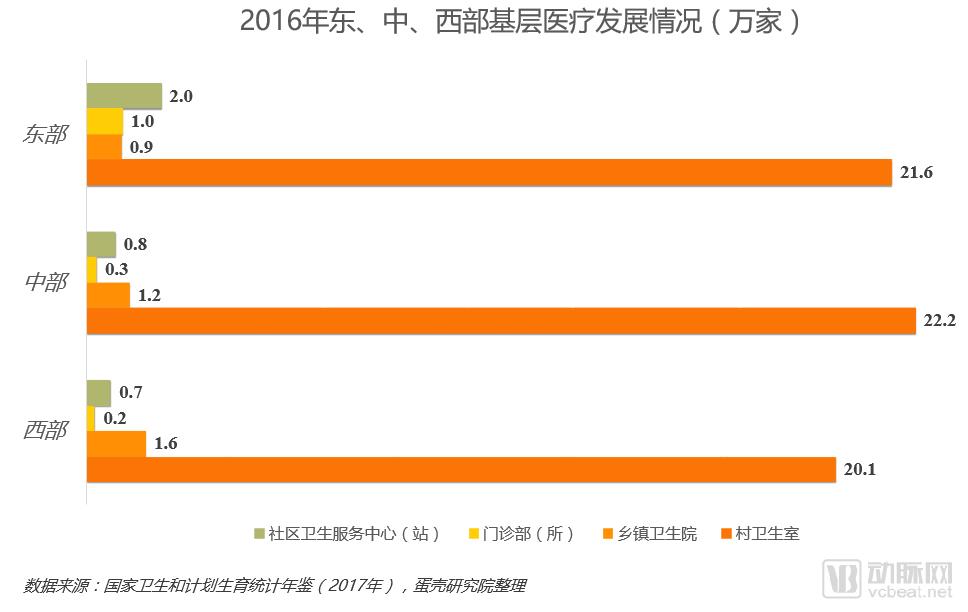
Pronounced Imbalance in Regional Development:Overall, primary healthcare in the eastern region is the most developed, followed by the central region, while the western region lags behind; this pattern is closely correlated with the level of regional economic development in China.
Village Clinics Have the Largest Number:Among various types of primary healthcare institutions in the eastern, central, and western regions, the number of village clinics far exceeds that of other types of institutions.
The Western Region Has the Largest Number of Township Health Centers:This is mainly due to the large number of townships in western provinces.
Lagging Development of Traditional Chinese and Western Medicine Outpatient Departments (Clinics):The number of outpatient departments and clinics in the central and western regions significantly lags behind that in the eastern region, primarily because most clinics are located in urban areas, and the eastern region has a greater number of cities than the central and western regions.
Bed and Equipment: Increased bed supply capacity, but insufficient equipment advancement

Scale Expands, Growth Slows:As the government has strongly supported the development of primary healthcare, the number and scale of primary healthcare institutions have expanded, leading to a significant increase in bed capacity. However, as the policy effects have diminished, the growth in the number of primary healthcare institutions has slowed, resulting in a corresponding decline in the rate of bed expansion.
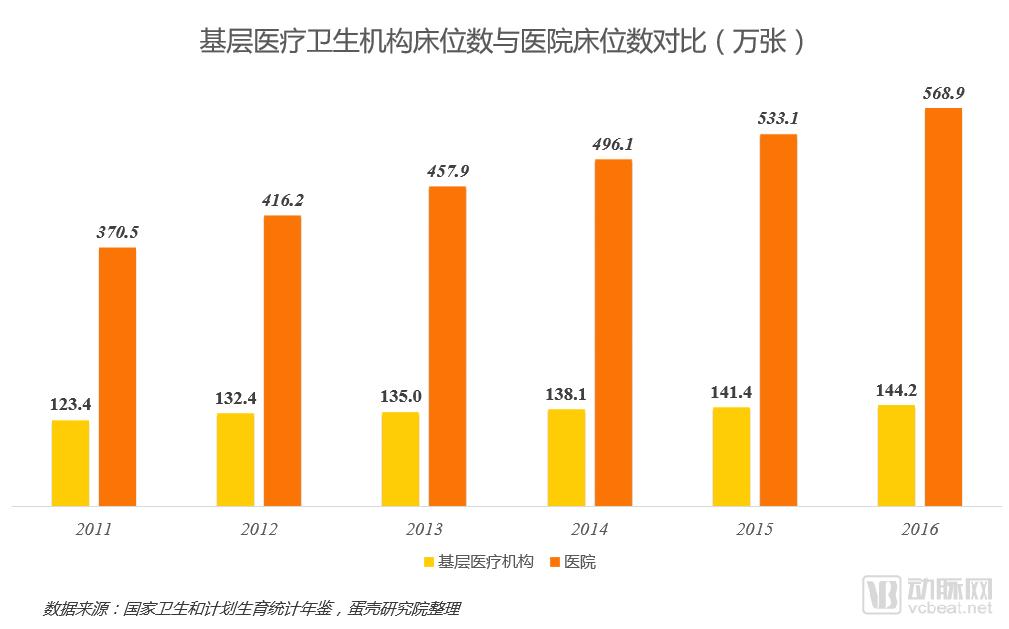
Bed counts are increasing:It indicates that both primary healthcare institutions and hospitals are continuously improving their medical service facilities.
The gap in total volume continues to widen:The gap in the number of beds between primary healthcare institutions and hospitals is widening, primarily because hospitals have a significant advantage in terms of financial support and funding strength. The government needs to further increase financial support for primary healthcare institutions, while these institutions themselves need to continuously enhance their financing capabilities and further improve service facilities.
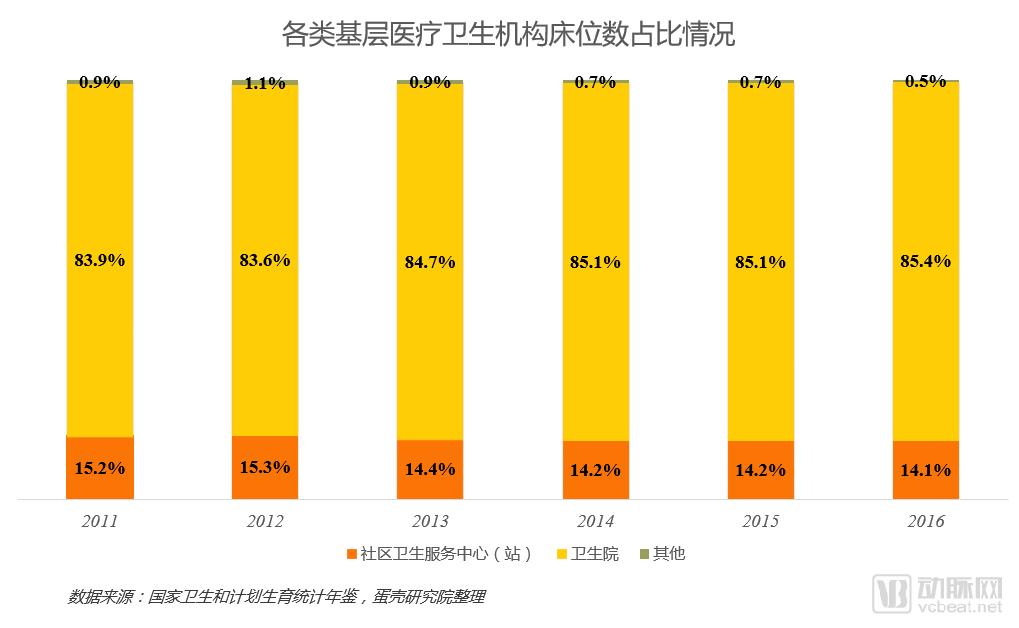
Township health centers account for the highest proportion of hospital beds, with their share expanding year by year, while the proportion of community health service centers (stations) is declining annually:This is mainly due to the decentralization of medical services, with township health centers becoming the primary providers of inpatient care at the grassroots level.
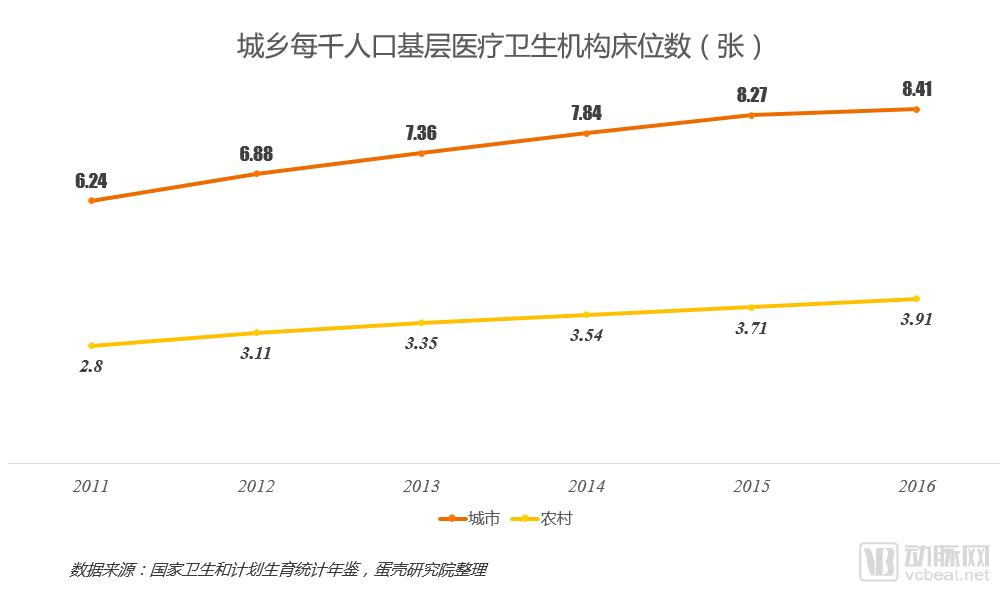
Increased Density of Primary Care Bed Supply:The number of hospital beds per 1,000 population has been increasing year by year, better meeting patients’ inpatient care needs.
Low Density of Rural Bed Supply:The number of beds per 1,000 people in primary healthcare institutions in rural areas is less than half that in urban areas, which is closely related to the lagging development of primary healthcare in rural regions. It is necessary to accelerate the development of rural primary healthcare and increase the density of bed supply in rural areas.
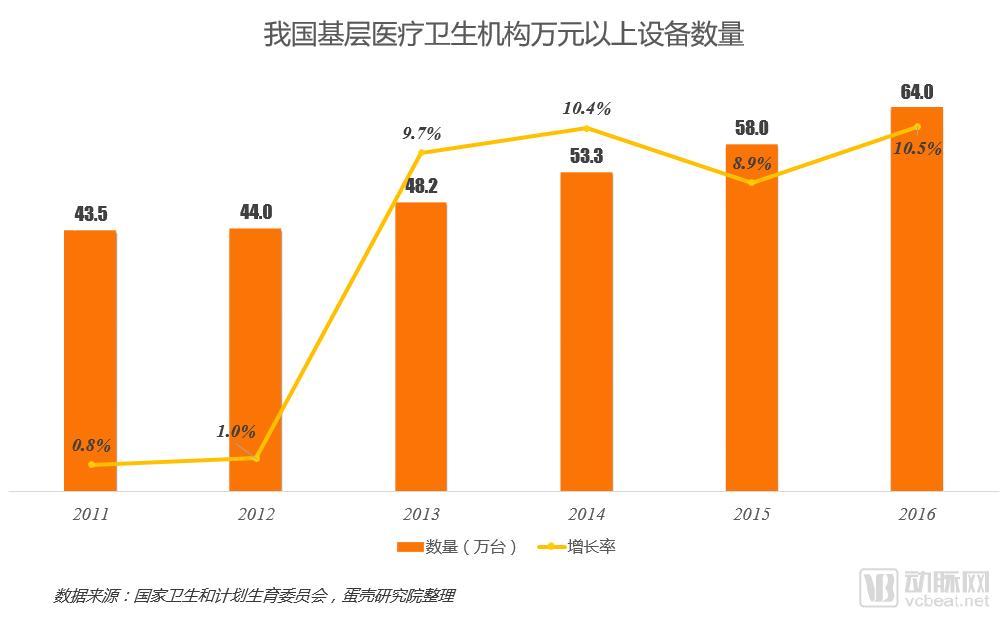
Hardware infrastructure is continuously improving and maintaining rapid growth:Strengthening equipment procurement and accelerating equipment upgrades in primary healthcare facilities help enhance diagnostic and treatment service capabilities. Notably, since 2013, the average annual growth rate of medical devices valued at over RMB 10,000 has reached as high as 9.9%. This progress is attributable to increased government subsidies for primary healthcare equipment.
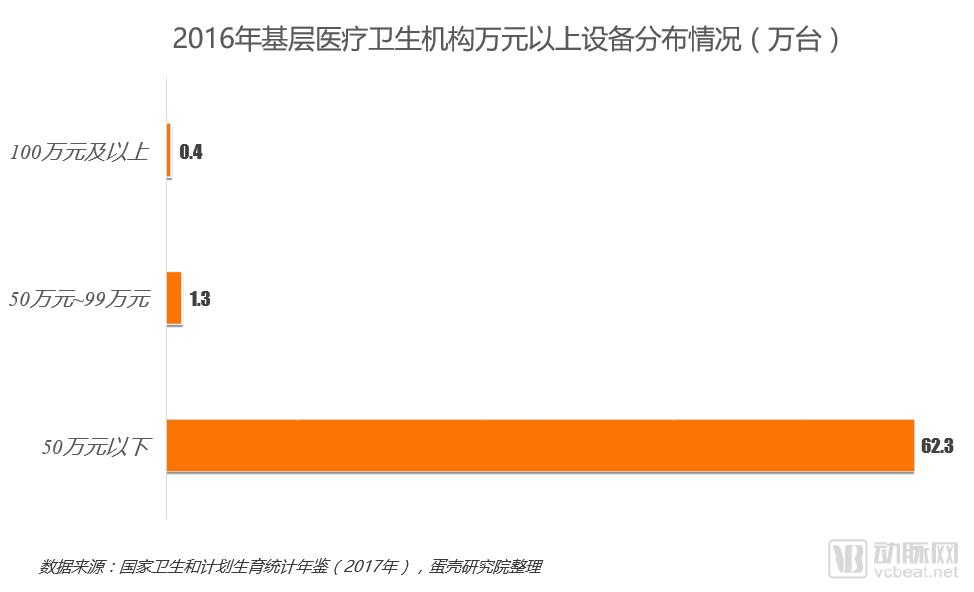
Insufficient Equipment Advancement:In China, medical equipment at primary healthcare institutions is predominantly valued below 500,000 yuan, with very few devices exceeding 1 million yuan. This indicates a low level of technological advancement, limiting their capacity to only the diagnosis and treatment of basic diseases, thereby necessitating the introduction of more advanced and higher-quality medical equipment.
Healthcare Personnel: Improved Quantity Supply, Structural Optimization Needed
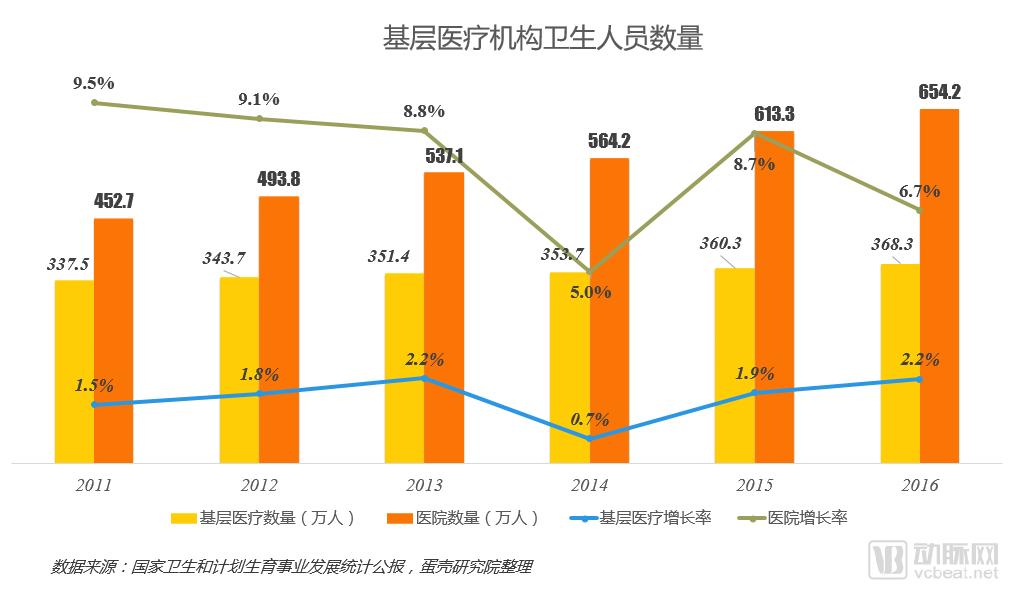
Increase in the Total Number of Health Personnel:The number of primary healthcare workers in China has been increasing year by year, helping to improve the capacity of primary healthcare services.
Imbalanced Distribution of Health Personnel:The majority of medical professionals are concentrated in hospitals, while the growth rate of healthcare workers at the primary care level remains low. This is primarily because hospitals offer stronger revenue-generating capabilities and better career development platforms, making them more attractive to talent.
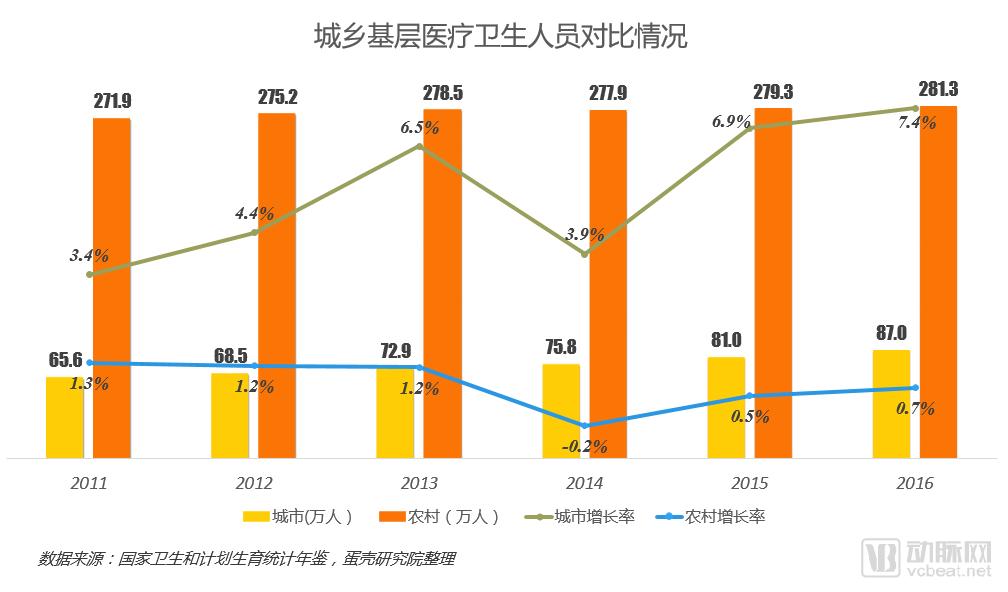
Severe Divergence in the Development of Urban and Rural Health Workforce:Urban areas have fewer facilities but higher growth rates, while rural areas have more facilities but slower growth. This is primarily because urban medical institutions offer better conditions and living environments than rural areas, making healthcare professionals more willing to stay and develop their careers in cities.
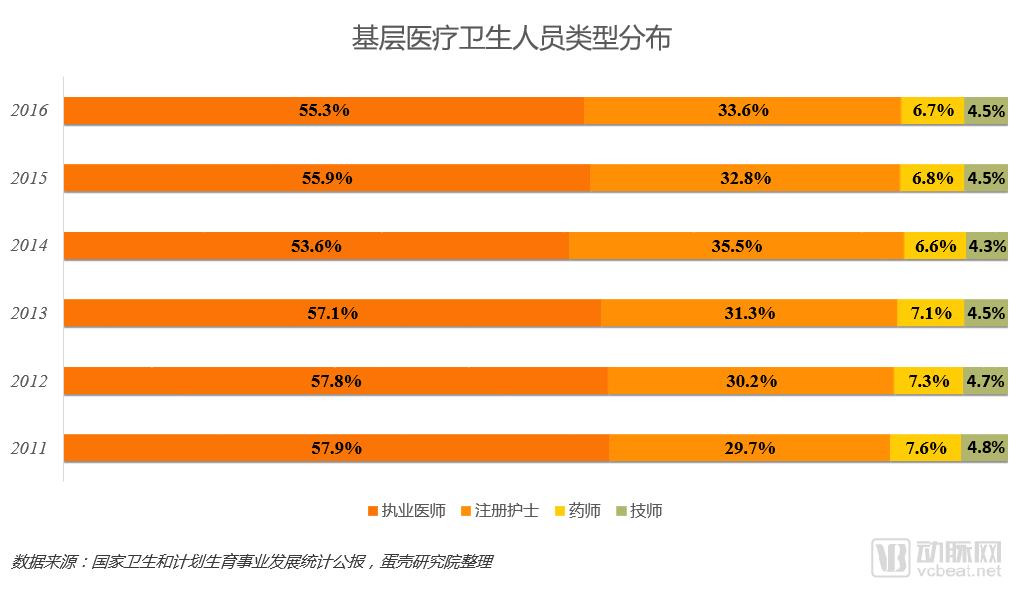
Highest proportion of physician resources:From the perspective of the proportion of health personnel in each year, the proportion of physicians has exceeded 50%, which provides a guarantee for the quality of primary medical services.
Shortage of Pharmaceutical and Technical Personnel:Among various types of personnel in primary healthcare, the proportion of pharmacists and medical technologists is relatively low. On one hand, physicians in primary care settings can perform the duties of pharmacists and technologists; on the other hand, there is an insufficient supply of qualified pharmacists and medical technologists in primary healthcare institutions.
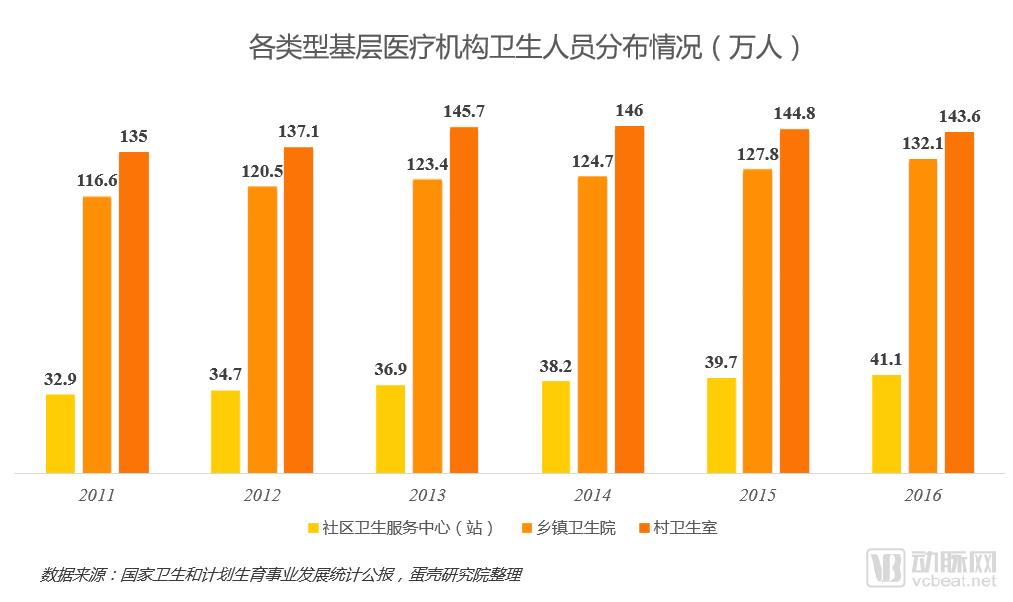
Village Clinics Have the Largest Number of Medical Personnel:China has a vast rural population, with the largest number of village clinics and medical personnel.
Divergent Development Trends:The number of medical personnel in township health centers and community health service centers (stations) has increased year by year, while the number of medical personnel in village clinics has decreased.
Service Performance: Highest Patient Volume, with Township Health Center Revenue Accounting for Half of the Total
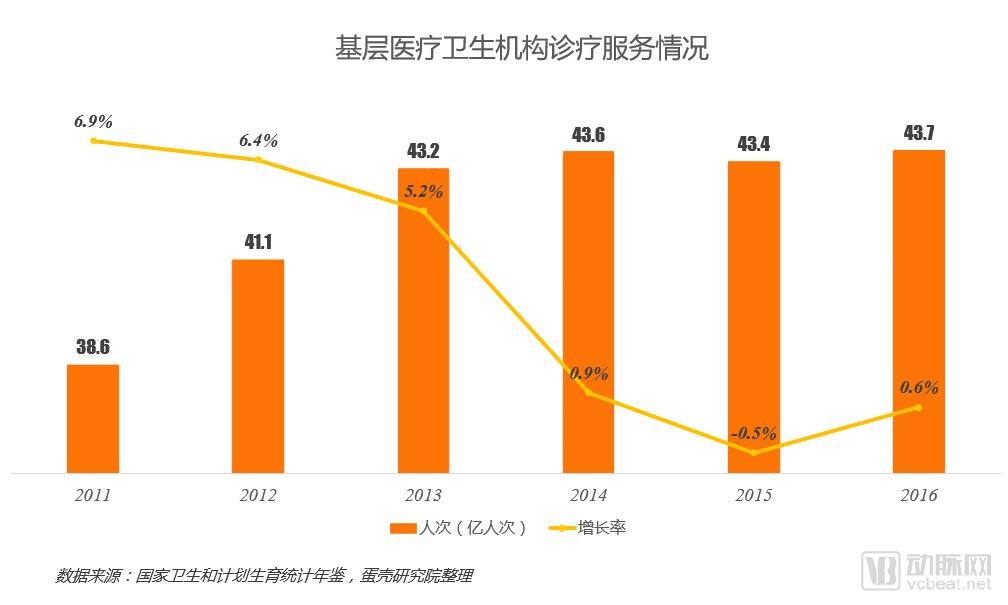
Highest Share of Patient Visits, but Sluggish Growth:The quality of primary healthcare services is inferior to that of hospitals, leading to a lack of patient trust in primary care and a preference for seeking treatment at hospitals.
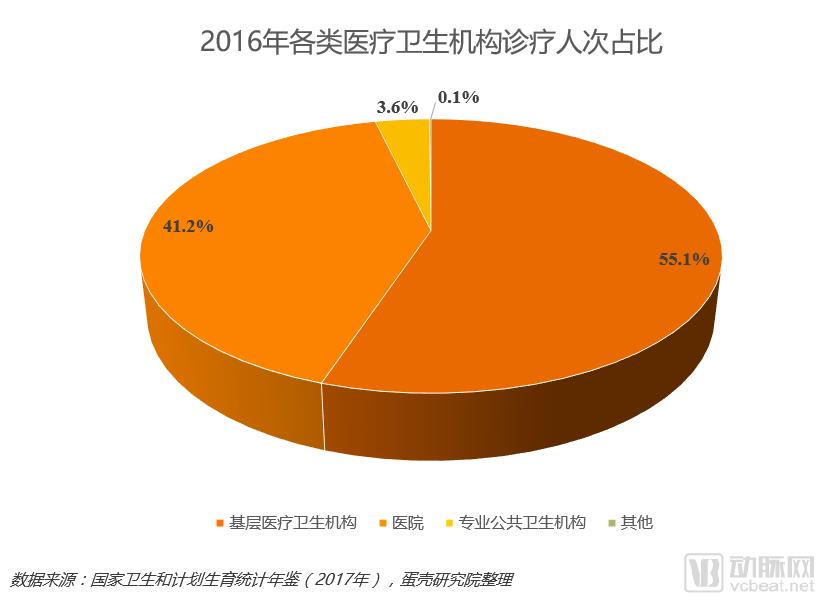
Mismatch Between Scale and Service Capacity:Primary healthcare institutions account for 95% of the total number of medical facilities, yet they handle only 55% of patient visits; in contrast, hospitals, which make up merely 3% of the total, account for a substantial 41.2% of patient visits. This disparity indicates an overcapacity in primary healthcare services and underscores the need to enhance public trust in primary care.
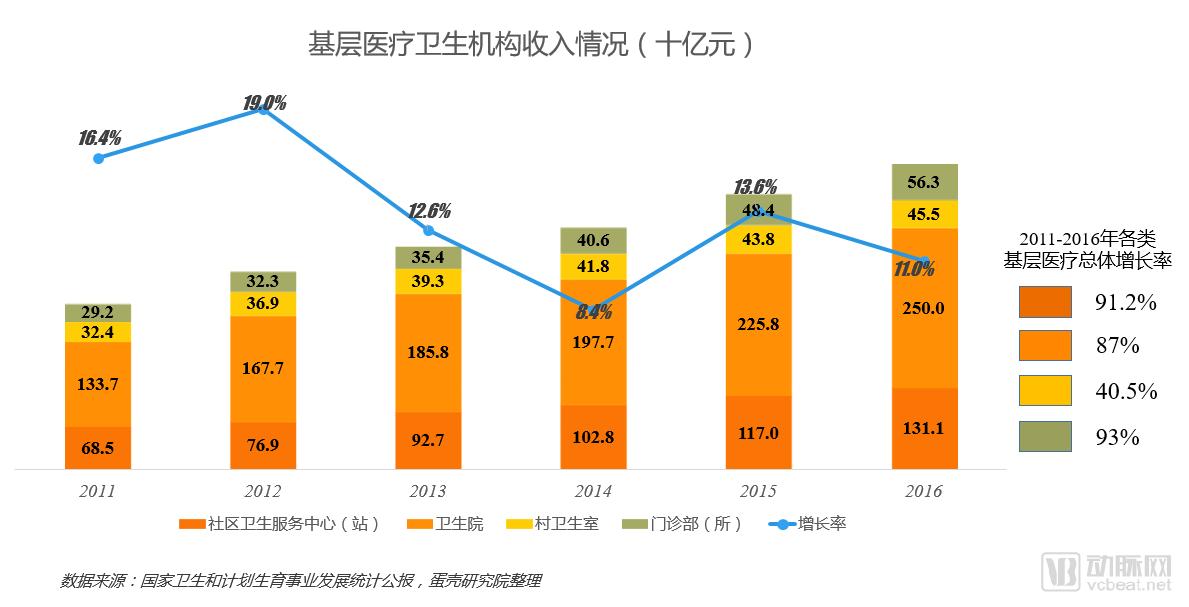
Total Volume Increases, Growth Rate Declines:Total revenue from primary healthcare has been rising year by year, but its growth rate has declined from 16.4% in 2011 to 11%. This is mainly due to the year-on-year decrease in the growth rate of patient visits at primary healthcare facilities.
Health Center Revenue Accounts for Half the Market:An analysis of the revenue of various types of primary healthcare institutions over the years shows that township health centers consistently account for more than 50% of the total. This is primarily attributed to their superior medical equipment and service capabilities compared to other primary healthcare providers, resulting in a higher volume of patient visits.
Weak Revenue-Generating Capacity of Village Clinics:Compared with other primary healthcare institutions, the revenue of village clinics has increased by only 40.5% over the past six years. This slow growth is primarily attributed to the rural-to-urban migration of the population and the relatively weak overall medical service capacity of village clinics.
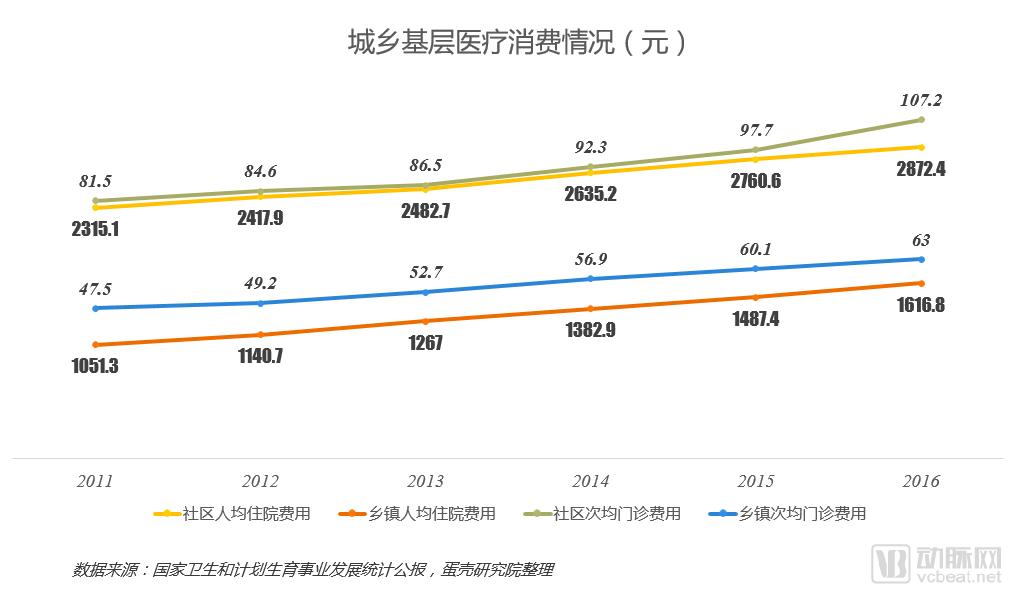
Resident Medical Expenditure Increases Year by Year:The rising per capita inpatient and outpatient expenses in communities and townships indicate a year-on-year growth in residents' healthcare consumption.
Inpatient costs are the main revenue generator:In community health centers and township hospitals, the average inpatient cost per capita is significantly higher than outpatient costs, making it the primary source of revenue for primary healthcare institutions.
The Huge Gap in Healthcare Consumption Between Urban and Rural Grassroots Areas:Per capita inpatient and outpatient expenses in urban communities are approximately twice those in township areas during the same period. This is primarily because urban residents have higher incomes and stronger healthcare payment capacity; meanwhile, their healthcare consumption concepts are keeping pace with the times, making them more willing to increase spending on health and medical care.。