ICU in the Face of Influenza: Technology and Compassion Safeguarding the Frontline of Life
By Li Qian
On January 12, the founder of a highly specialized vertical medical media outlet whom I admire asked me about ECMO and its prognosis at the request of his former colleague.
In my view, ECMO is currently widely used, and the technology is relatively mature. At that time, four ECMO machines were running simultaneously in the Respiratory Intensive Care Unit (RICU) of Chaoyang Hospital, which served as the clinical trial site for our product (the Intelligent Bionic Sputum Excretion System). Since a friend mentioned that the patient was hospitalized at China-Japan Friendship Hospital, I looked up several articles on ECMO use at that institution—China-Japan Friendship Hospital has already performed over one hundred ECMO cases. I also advised him that, as extracorporeal circulation inevitably carries risks of complications, it is best to follow the treating physicians’ recommendations.
Later, the viral article “A Beijing Middle-Aged Man’s Journey Through Influenza” flooded social media feeds, and I realized that the person who had inquired about me through a friend at the time was none other than the author. After reading the piece and witnessing its ultimately regrettable outcome—the patient’s suffering and the harrowing description of blood gushing uncontrollably after the tubes were removed—I find myself wondering whether I would still offer the same recommendation if given the chance to do it all over again.
That article served as a genuine lesson on influenza, a case study in medical ethics, and an education on mortality. As the founder of an innovative medical device company specializing in respiratory care, I have maintained close ties with intensive care units (ICUs) since the company’s inception: identifying pain points within ICUs, collaborating with ICUs at renowned hospitals, learning from ICU practices, and conducting clinical trials of our developed devices in ICU settings. Over the past few years, I have visited ICUs countless times and directly collaborated with more than ten of them. The authentic and detailed portrayal of patients’ worlds presented in the article has once again profoundly moved me.
For the average person, a visit to the ICU is sure to be deeply moving; life and death are commonplace there.
"My first visit to an ICU was at the Emergency ICU of Beijing Hospital. I saw patients lying in bed like fallen leaves, their limbs withered and dry, with only their hands swollen into round shapes—a deeply shocking sight."
Outside an ICU, doctors issued several critical condition notices to the family of a lung cancer patient. The patient’s daughter and younger sister wept continuously, yet his wife remained dry-eyed. It later became clear that those who must clean up the aftermath cannot afford to cry, while those clinging to a sliver of hope will not believe in a bad outcome until the very last moment.
During daily visiting hours, family members queue up outside the ICU as if it were a festival, prompting an involuntary reflection on one’s own end of life and how one would respond.
Of course, our team has also witnessed such stories.
An elderly female ICU patient with amyotrophic lateral sclerosis (ALS) has been hospitalized in the intensive care unit for several years. Despite being trapped in a disabled body, she retains clear consciousness. Under comprehensive medical treatment and nursing care, she uses an iPad daily to binge-watch TV series. The medical staff must keep track of which episode she has last watched; otherwise, she becomes quite upset.
An elderly patient, though fully conscious, required the doctor to patiently explain the use of each therapeutic device; otherwise, he would become panicked and resistant. After every session with our sputum clearance machine, the doctor would gently ask if he felt more comfortable. The moment they saw him nod, our team members said they instantly felt a profound sense of meaning in their work.
As a driving force behind the R&D of innovative medical devices, we should emulate physicians by exercising rational compassion and, from an ethical perspective, striving to alleviate patients’ suffering and reduce the burden on their families. This has always been our approach: making innovation and compassion the keywords of our corporate culture, and leveraging innovative technologies and a compassionate heart to help patients.
“A Beijing Middle-Aged Man’s Journey with Influenza” has drawn widespread public attention to influenza and the intensive care unit (ICU). Here, I share some of my preliminary insights, guiding readers through the ICU from the perspectives of influenza, pneumonia, and medical devices.
I reviewed some information on influenza. According to the World Health Organization, seasonal influenza causes 3–5 million cases of severe illness and 300,000–500,000 deaths worldwide each year. In the United States alone, influenza leads to 140,000–170,000 hospitalizations and 12,000–56,000 deaths annually, making it the disease with the highest burden among children, the elderly, and individuals with multiple comorbidities.
The current influenza season is predominantly driven by the H3N2 subtype, with co-circulation of H1N1 and influenza B viruses. According to statistics from the Australian Department of Health, there were 215,280 reported cases by mid-October, far exceeding the 59,022 cases recorded during the 2009 H1N1 influenza pandemic. The majority of these cases were caused by the H3N2 virus, and preliminary estimates indicate that the vaccine effectiveness against H3N2 was only 10%.
Throughout the winter, several ICUs where we conducted clinical work continuously admitted patients with severe influenza. By late December 2017, more than half of the patients in one ICU were suffering from severe influenza. In early January, we embarked on a new round of clinical training; at that time, one-third of the medical staff at the Chaoyang Respiratory Intensive Care Unit (RICU) had already contracted influenza once yet remained on the front lines. Over the course of a week, my colleagues and I visited four or five ICUs consecutively, unaware of fear at that time.
Classified by pathogen, pneumonia can be categorized into bacterial pneumonia, viral pneumonia (caused by SARS virus, avian influenza virus, influenza virus, etc.), and atypical pneumonia (such as Mycoplasma pneumonia, Chlamydia pneumonia, Legionnaires' disease, etc.). With the invention of antibiotics, pneumonia may seem less formidable than before, but many cases still pose significant challenges for physicians.
Liu Youning, former Chairman of the Respiratory Branch of the Chinese Medical Association, once stated: “More than half of patients with chronic illnesses die from pneumonia. For many individuals with chronic conditions, such as diabetes and stroke, as well as the elderly and frail, the immediate cause of death is ultimately pneumonia. Among hospitalized patients with chronic diseases, pneumonia accounts for more than half of all deaths.”
Ventilator-Associated Pneumonia (VAP) is a relatively common complication in the ICU, defined as pneumonia that develops more than 48 hours after the initiation of invasive mechanical ventilation. VAP is closely associated with the inability to promptly and effectively drain deep pulmonary secretions. Domestic literature reports a VAP prevalence rate of 43.1% and a mortality rate of 51.6%. Some high-performing ICUs have managed to reduce VAP incidence to lower levels.
Furthermore, contracting drug-resistant bacteria in a hospital can be extremely troublesome, as exemplified by the father-in-law in the article “Beijing Middle-Aged Man Under the Flu.”
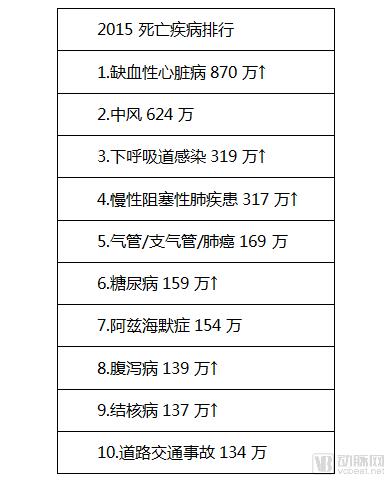
Based on the global rankings of causes of death in 1990, 2013, and 2015, pneumonia has consistently ranked among the top three or four [2]. Respiratory diseases have steadily occupied four of the top ten spots, namely pneumonia/lower respiratory infections, chronic obstructive pulmonary disease (COPD), tracheal/bronchial/lung cancer, and tuberculosis.
Based on these data, we have every reason to assert that respiratory health should take the lead in the "Healthy China" initiative, and we hope to see growing public attention paid to respiratory diseases. What is the current state of medical devices in light of this severe situation? The respiratory device sector is characterized by a limited variety of products, slow technological advancement, and a low market share of domestically manufactured devices. It is against this backdrop that we focus on the innovation, research, and development of airway management and respiratory therapy devices, aiming to provide clinicians with more effective tools and contribute to the advancement of this industry.

"World Health Statistics 2017"[4]

High-flow oxygen therapy has been developed abroad for more than ten years. It was introduced to China in 2012. Currently, the main high-flow oxygen therapy devices include Venturi masks and nasal high-flow oxygen therapy devices. The currently widely used device is the nasal high-flow oxygen therapy device, which directly delivers a high flow of air-oxygen mixture with a specific oxygen concentration to patients through an unsealed nasal cannula. At the same time, it is equipped with active heating and humidification functions. Nasal high-flow oxygen therapy equipment can provide an oxygen concentration of 21-100%, allowing precise oxygen delivery. It has a dead space flushing effect, provides fully heated and humidified gas, protects airway mucosa and cilia, reduces upper respiratory tract resistance and breathing effort, and generates low-level positive airway pressure. Patients experience better comfort and compliance. Its clinical application range is extensive, and its effectiveness is significantly superior to conventional oxygen therapy. It can serve as a bridge between non-invasive ventilation and routine oxygen therapy.
Ventilators are devices that can replace, control, or modify a person’s normal physiological respiration. They increase pulmonary ventilation, improve respiratory function, reduce the work of breathing, and conserve cardiac reserve. Thanks to technological advancements, ventilator performance has become increasingly sophisticated, evolving from the early negative-pressure “iron lung” to today’s multifunctional, computer-controlled models. Their applications have expanded significantly, and therapeutic outcomes have continued to improve. Based on the method of connection between the ventilator and the patient, ventilation is primarily categorized into non-invasive ventilation and invasive ventilation.

Non-invasive ventilation refers to a mode of positive pressure ventilation in which the ventilator is connected to the patient via an oral or nasal mask, without the need for intubation or establishment of an invasive artificial airway. Non-invasive ventilation was initially applied as an adjunctive therapy for sleep apnea syndrome, significantly improving patients’ mental status and sleep quality, and preventing complications such as stroke and cardiopulmonary dysfunction.
Invasive ventilation refers to mechanical ventilation delivered via an artificial airway (endotracheal intubation or tracheostomy tube). As one of the most critical life-support techniques in clinical practice, invasive positive pressure ventilation was first introduced into clinical use in the 1950s and has entered a relatively mature stage over the past decade. Invasive mechanical ventilation is indicated when conventional oxygen therapy or non-invasive ventilation support yields inadequate results.
Ko Wen-je (formerly a surgical intensive care physician at National Taiwan University Hospital and a professor at National Taiwan University College of Medicine, currently the Mayor of Taipei) stated in his TED Talk, “The Wisdom of Life and Death,” that there are only two outcomes in life: intubation or no intubation, highlighting the importance and ubiquity of mechanical ventilation.
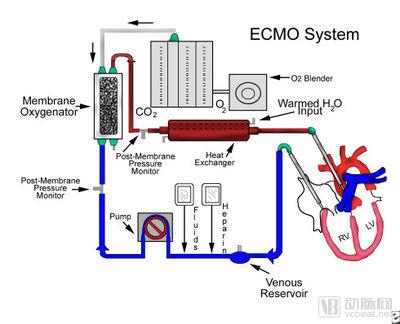
Extracorporeal Membrane Oxygenation (ECMO), also known as ECMO, is an improved artificial heart-lung machine. Its core components are the membrane oxygenator and the blood pump, which function as an artificial lung and an artificial heart, respectively [4-5]. During ECMO operation, blood is drained from the veins, passes through the membrane oxygenator to absorb oxygen and eliminate carbon dioxide. The gas-exchanged blood can then be returned either to the veins (VV pathway) or to the arteries (VA pathway) under the propulsion of the pump.
The former is primarily used for extracorporeal respiratory support, while the latter, whose blood pump can substitute for the heart’s pumping function, serves both extracorporeal respiratory support and cardiac support. When a patient’s pulmonary function is severely impaired and unresponsive to conventional therapy, ECMO can assume gas exchange duties, allowing the lungs to rest and buying valuable time for recovery. Similarly, when cardiac function is severely compromised, the blood pump can take over the heart’s pumping role to maintain circulation.
In terms of the intensity of life support provided to patients, the modalities range from weakest to strongest as follows: high-flow oxygen therapy → non-invasive ventilation → invasive mechanical ventilation → ECMO. From this perspective, ECMO is indeed the ultimate life-saving device in the ICU.
Most patients admitted to the ICU require endotracheal intubation or tracheostomy, necessitating inevitable monitoring of cuff pressure. The endotracheal tube cuff provides a seal to prevent air leakage during mechanical ventilation and to avoid aspiration of oropharyngeal secretions and gastroesophageal refluxate into the lungs, which can lead to pneumonia.
The Clinical Practice Guidelines for Mechanical Ventilation stipulate that cuff pressure should be maintained at 20–30 cmH2O; insufficient pressure poses risks of air leakage and aspiration, while excessive pressure can cause pressure necrosis of the airway wall [6]. Surveys conducted both domestically and internationally indicate that most anesthesiologists and emergency physicians still rely on the finger palpation method to empirically assess whether the cuff is adequately inflated. This approach often leads to overinflation, with cuff pressures reaching as high as 154 cmH2O, even among highly experienced physicians [7].
Currently, the most commonly used devices are mechanical manometers and electronic manometers. Compared with traditional mechanical manometers, electronic manometers offer simpler operation, digital display, real-time monitoring of cuff pressure, and high measurement accuracy. They can automatically alert when the pressure is too high or too low, thereby preventing air leakage during operation and minimizing the workload of healthcare professionals. These devices have been included in the textbook *Integrative Traditional Chinese and Western Medicine in Emergency Care*.

Most patients receiving invasive mechanical ventilation in the ICU are in a comatose state and have minimal cough reflex, often requiring suctioning to clear secretions and maintain airway patency. Effective airway management and timely removal of respiratory secretions are essential to maintain ventilation and adequate gas exchange, effectively prevent pulmonary infections, and reduce the duration of mechanical ventilation. Suctioning is the most frequently performed procedure for ICU patients undergoing mechanical ventilation. Suction catheterization is a manual technique in which a suction catheter is inserted into the main airway and connected to negative pressure to aspirate secretions encountered by the catheter. Suction catheters are classified into open and closed systems.

Open suction catheters consist of two components: the suction tubing and the machine-end connector. With a simple structure and ease of operation, they represent the predominant method of suctioning currently employed in clinical practice. However, their use requires disconnection from the ventilator circuit, which can readily induce choking or coughing in patients and may even cause sputum to splash onto the faces and bodies of healthcare workers, posing an occupational hazard. Furthermore, after suctioning, the exposed suction tubing is susceptible to environmental contamination, thereby increasing the risk of ventilator-associated pneumonia (VAP).
Closed Suction CatheterThe closed suction catheter consists of three parts: the patient end, the catheter body, and the machine end. The patient end connects to the artificial airway and mechanical ventilation system, and also allows for medication administration. The catheter body is composed of a suction tube encased in a plastic film, which isolates the circuit from the external environment. The machine end connects to the suction device to facilitate negative pressure operation. Closed suction catheters began to be used in clinical practice in China in the late 20th century. The original intention behind the closed suction design was to prevent the airborne dissemination of bacteria-laden droplets by relatively isolating the suction circuit from the external environment, thereby effectively protecting both patients and healthcare workers. During the SARS epidemic, it effectively protected healthcare workers from infection.

Vibratory expectoration device is a mechanical instrument that utilizes the principle of physical vibration to replace manual back percussion by nurses, thereby facilitating the expulsion of pulmonary sputum. It helps loosen sputum crusts and also promotes sputum expectoration.

Intelligent Bionic Sputum Expectorator (Bionic Cough Simulator) is an intelligent device that simulates physiological human coughing, enabling patients to safely and efficiently clear deep pulmonary secretions through coughing, similar to healthy individuals. It can operate in parallel with a ventilator using time-sharing coordination. After the ventilator delivers a complete inspiratory breath to the patient, the intelligent bionic expectoration function is activated. By mimicking the human cough mechanism, it generates a brief high-flow air burst that directly expels sputum from the main airways and bronchi during exhalation. This system effectively clears deep lung secretions. Its intelligent sensor system ensures automatic switching of the airway between the ventilator and the expectorator, guaranteeing both safety and efficacy. This product will be launched soon to benefit more patients.
Of course, there are also vital signs monitors, blood gas analyzers, cardioverters, defibrillators, temporary pacemakers, blood purification systems, electrocardiographs (ECG machines), and other equipment. Due to space constraints, they will not be described individually.
ICU beds generally account for 2% to 8% of a hospital’s total bed capacity; developed countries approach the upper end of this range, while we remain close to the lower end. With technological advancements, ICU cure rates are steadily increasing (some literature reports rates as high as 80%, though actual figures may be somewhat lower), meaning an ICU admission no longer signifies hopelessness. As the final line of defense in saving patients’ lives, ICUs are equipped with increasingly sophisticated medical devices. It is hoped that more “game-changing” tools will become available to clinicians and that domestically produced medical devices will gain greater market share. Many patients stay in the ICU for several days postoperatively, while a significant number of long-term patients reside there for extended periods (over one year).
As innovators in healthcare during the digital age, our mission is to leverage innovative technologies and compassionate care to develop more tools for physicians and nurses, address clinical pain points, alleviate patient suffering and reduce the burden on families. We strive to accompany patients through the darkest periods of their lives, guiding them out of isolation and hardship so they may reunite with their loved ones. Every patient who uses our devices inspires us to move forward. Our goal is to become a superior partner in intelligent airway management and respiratory therapy, providing robust support for the development of better ICUs, until that inevitable day arrives.
Wishing everyone the ability to work healthily for our motherland for 50 years!
References:
[1] Catharine I,Paules MD,Sheena G,et al.Chasing Seasonal Influenza—The Need for a Universal Influenza Vaccine.N Engl J Med. 2018;378:7-9.
[2] HME GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet, Dec 18,2014 DOI: 10.1016/S0140-6736(14)61682-2).
[3] World Health Statistics 2017.
[4] Ko Wen-je: The Wisdom of Life and Death
[5] Regina Phelps.H1N1 (Swine Flu): Preparing for the Sickest of the Sick – Three Studies of ICU Treatment of Critically Ill H1N1 Patients.JAMA. 2009;302(17):(doi:10.1001/jama.2009.1539)
[6] Clinical Practice Guidelines for Mechanical Ventilation 2006.
[7] Expert Consensus on the Management of Artificial Airway Cuffs (2016).

About the Author:Founder and CEO of Yaguo Technology, a senior medical device expert who graduated with a major in Signal Processing from the Chinese Academy of Sciences and completed the Singularity University Global Solutions Program. Yaguo Technology focuses on innovation in airway management and respiratory therapy, aiming to be a superior partner in intelligent airway management and respiratory care. The company’s Intelligent Bionic Sputum Excretion System was recognized as a Moonshot project by Google X and the AAAS; its Respiratory Neuromuscular Stimulator for chronic respiratory failure rehabilitation was designated as an Innovative Medical Device by the Beijing Medical Products Administration; and its domestically produced first continuous cuff pressure monitoring product has been included in the 13th Five-Year Plan textbooks for emergency and critical care in both traditional Chinese and Western medicine.