Accessing Medical Insurance Payment Systems for Clinics: A Comparative Review of Procedures and Requirements Across Six Major Chinese Cities
For most grassroots clinic entrepreneurs, whether to integrate with medical insurance payment systems is crucial.
“As soon as Jiaxing Community Chain Clinics was established, I integrated medical insurance payment services to earn the trust of local residents,” Li Changjiang, founder of Chongqing Jiaxing Medical, told VCBeat.
According to Xu Dan, Investment Director at Shanghai Tongjiang Capital Investment Group Co., Ltd.: “The core of community clinics lies in their integration with the national medical insurance system. They can serve as an initial customer acquisition channel, drawing residents in by providing tangible, beneficial services that build trust and generate positive word-of-mouth, thereby attracting more users. This will also become a criterion for us in identifying investment targets and deciding whether to invest in a project.”
In Hangzhou, thousands of kilometers away from Chongqing, medical institutions such as clinics and outpatient departments have also actively integrated with national health insurance payment systems. For instance, DXY Clinic enabled health insurance payments in April 2017; four months later, WeDoctor General Practice Center also connected to the health insurance payment system in Xiaoshan District.
These cases may create the illusion that it is easy for clinics to integrate with medical insurance payment systems. In reality, this is precisely a major pain point for clinics, dampening the enthusiasm of many clinic entrepreneurs. Due to high thresholds, stringent approval processes, and prolonged timelines, countless clinics are shut out. As a result, any mention of applying for designated medical insurance provider status seems to evoke endless hardships for clinics.
How long does the entire process of connecting a clinic to the medical insurance payment system take? What procedures are required? What are the criteria for medical insurance accreditation? Are the access standards consistent across different regions?
With these questions in mind, VCBeat (WeChat ID: vcbeat) searched public records and examined the processes for clinics in six cities—Beijing, Shenzhen, Hangzhou, Chengdu, Tianjin, and Chongqing—to enroll in the medical insurance payment system. We hope this provides some guidance to clinic founders.
In fact, on May 11, 1999, to implement the Decision of the State Council on Establishing the Basic Medical Insurance System for Urban Employees (Guo Fa [1998] No. 44), the Ministry of Labor and Social Security, the Ministry of Health, and the State Administration of Traditional Chinese Medicine jointly formulated the Interim Measures for the Administration of Designated Medical Institutions under the Basic Medical Insurance System for Urban Employees (hereinafter referred to as the “Measures”).
The Measures refer to designated medical institutions, which are defined as healthcare facilities that have been reviewed by the labor and social security administrative department of the pooling region and approved by the social insurance agency to provide medical services to participants in the basic medical insurance for urban employees.
The principles for the review and designation of medical institutions are as follows: to facilitate medical access for insured individuals and streamline administration; to balance specialized and general care, as well as traditional Chinese medicine and Western medicine, while emphasizing the role of community health service institutions; to promote the optimized allocation of healthcare resources, improve the utilization efficiency of healthcare resources, reasonably control healthcare service costs, and enhance the quality of healthcare services.
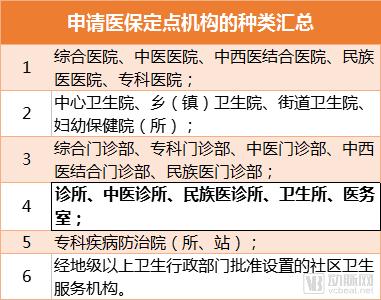
Which institutions are eligible to apply for designated status under the medical insurance scheme (medical insurance payment)? First, medical institutions that have been approved by the health administrative authorities and have obtained the Medical Institution Practice License, as well as military medical institutions authorized by the relevant military authorities to provide external services. As shown in the figure:
Clinics applying for medical insurance reimbursement must also meet the following requirements: comply with regional healthcare facility planning and healthcare institution accreditation standards; abide by national laws, regulations, and standards governing medical service administration, and maintain sound and comprehensive medical service management systems; strictly implement pricing policies for medical services and pharmaceuticals as stipulated by national and provincial (autonomous region, municipality directly under the Central Government) price control authorities, and pass supervision and inspections conducted by these authorities; strictly adhere to relevant policy provisions of the Basic Medical Insurance System for Urban Employees, establish internal management systems compatible with basic medical insurance administration, and staff necessary managerial personnel and equip essential facilities.
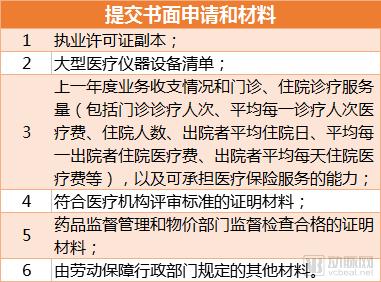
When a clinic is willing to serve as a designated medical institution for the Basic Medical Insurance for Urban Employees, it shall submit a written application and relevant materials to the labor and social security administrative department of the pooling region.
The most critical point mentioned in the Measures is: “The labor and social security administrative departments of each province (autonomous region, municipality directly under the Central Government) may, in accordance with these Measures, organize relevant departments such as health to formulate detailed implementation rules. These Measures shall come into force on the date of promulgation.”
The reality is that although policies were reissued across China based on local conditions, reflecting the framework of national regulations, the number of clinics integrated into the medical insurance payment system has remained limited. In contrast, hospitals and pharmacies have seen much higher integration rates. Anhui Province has been the fastest in promoting this initiative; by 2012, clinics in cities such as Xuancheng and Hefei had already been connected to the medical insurance payment system, while Wuhu City lagged significantly behind in achieving integration.
In October 2016, Meng Qingyuan of Yuanyang County People’s Hospital in Henan Province stated, “With the advancement of the new healthcare reform, and considering the overall design as well as China’s current medical system and practical healthcare needs, it is an inevitable trend and imperative to include individual medical practices in the medical insurance scheme; it is only a matter of time.”
The General Office of the State Council’s “Several Policy Measures on Promoting the Accelerated Development of Socially Run Medical Institutions” stipulates that such institutions shall be included in the designated reimbursement network of basic medical insurance, and that ownership structure shall not be used as a prerequisite for designation. This demonstrates the government’s high priority attached to socially run medical care and its intention to create favorable conditions. By encouraging greater private capital investment in healthcare and increasing both the quantity and quality of private medical institutions, the government aims to leverage the “catfish effect” to improve and advance the optimal allocation of medical resources, thereby alleviating the difficulties and high costs associated with accessing medical care.
Meanwhile, individual clinics possess both legal qualifications and the advantages of simplicity and efficiency. Compared with public hospitals and private medical institutions, they differ only in terms of operational context, funding, structural composition, and service volume, while still maintaining qualified professional capabilities to provide services under the medical insurance system. Integrating individual clinics into the medical insurance payment system will help alleviate the healthcare burden on patients served by village clinics and village doctors, drive and promote the rational reallocation of medical resources at the primary care level, and thereby enhance the overall comprehensive medical standards of primary healthcare.
These clinics emerged in a market economy environment, with competition ingrained in their very DNA. They provide affordable, high-quality medical services to society and have established a strong foundation of trust with consumers. Possessing an in-depth understanding of regional sociocultural and geographic characteristics, as well as the healthcare needs of special populations, and being designated as medical insurance providers, these clinics are well-positioned to leverage their strengths. While delivering high-quality basic medical services, they have the capability, resources, and competitive advantage to actively engage in regional public health initiatives, chronic disease management, geriatric health examinations, and health education campaigns. In particular, they hold distinct advantages and superiority in implementing family physician contract services, owing to the favorable relationships and atmosphere they have long cultivated with their patients.
Whether considering the qualifications, conditions, and capabilities of clinics, or the aspirations of individual practitioners and their surrounding communities, especially given the immense pressure currently facing the government to implement a tiered diagnosis and treatment system, it is evident that incorporating individual medical practices into the national health insurance scheme is an inevitable trend and aligns with the healthcare-seeking needs of the grassroots population.
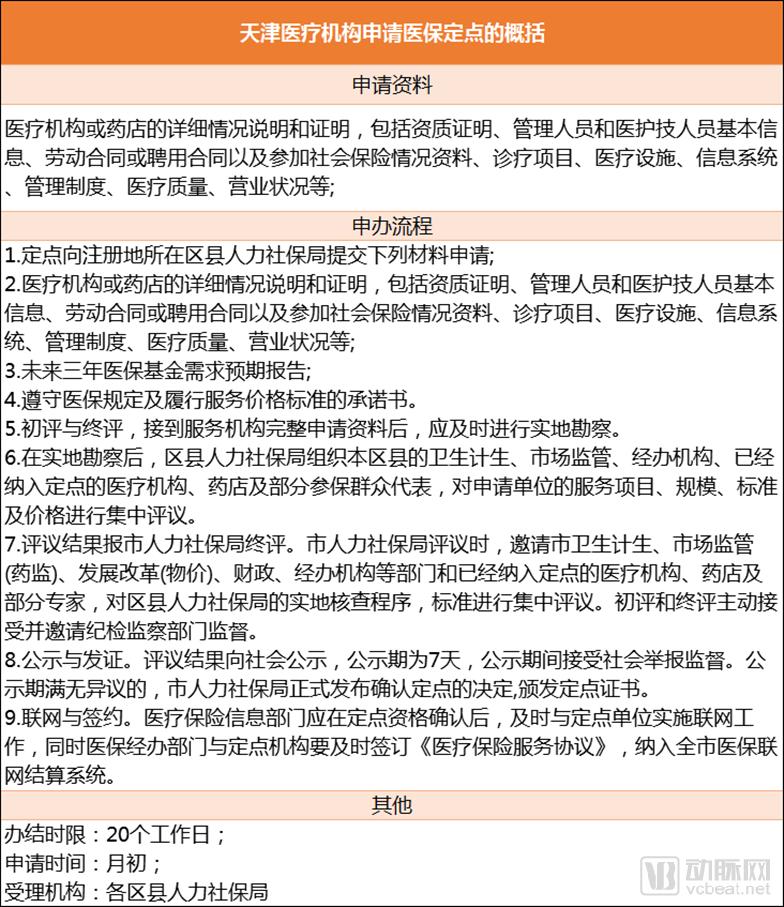
Subsequently, regions across China introduced a series of interim regulations on medical insurance supervision, tailored to local conditions, with the aim of enabling primary care clinics to participate in medical insurance payment systems. As shown in the figure:
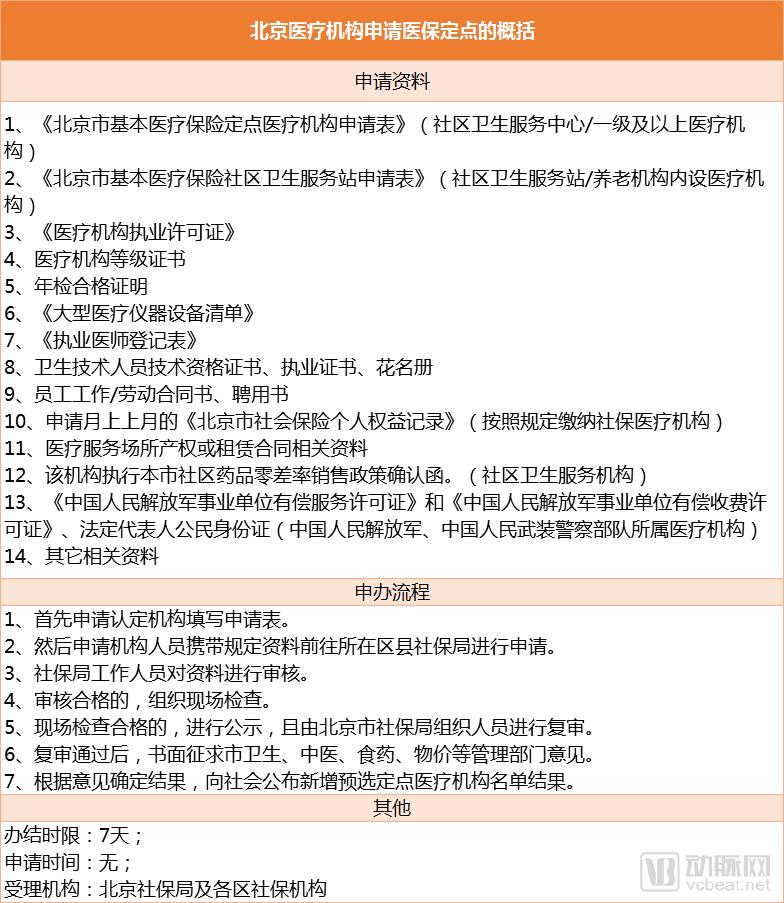
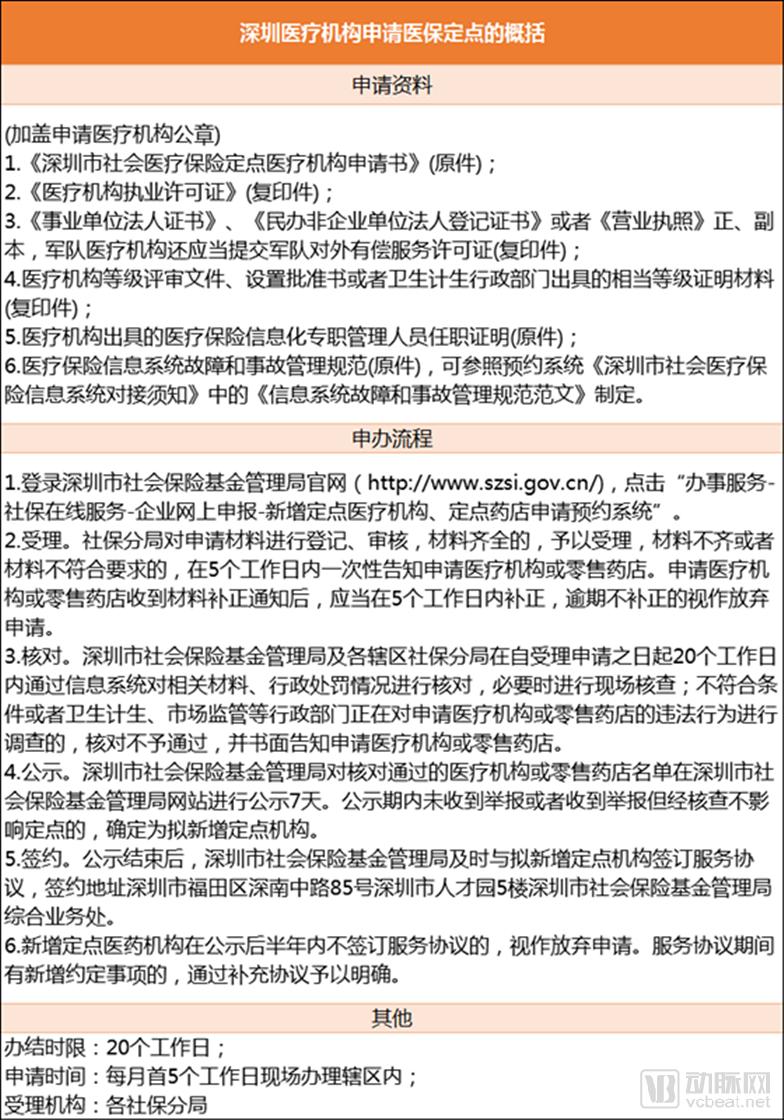
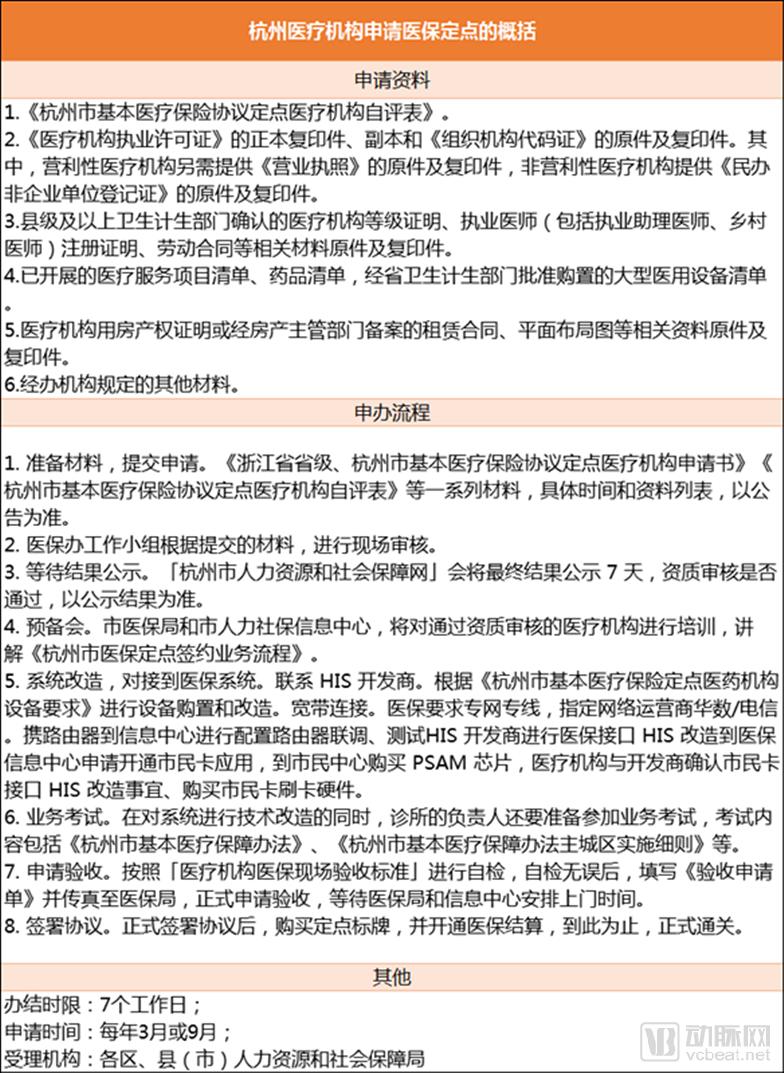
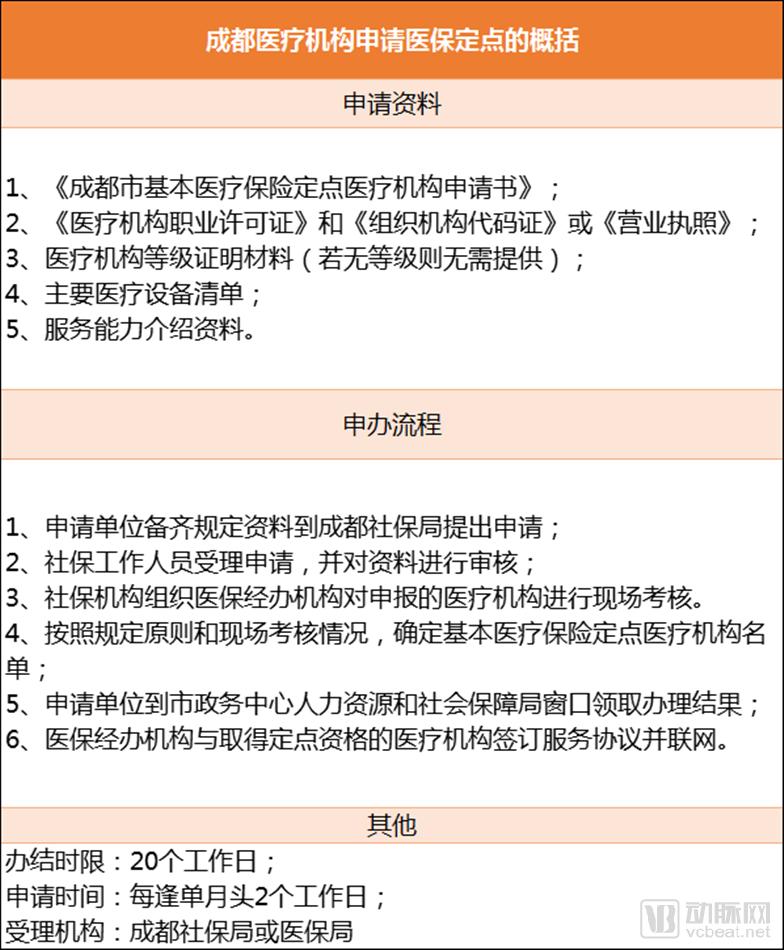
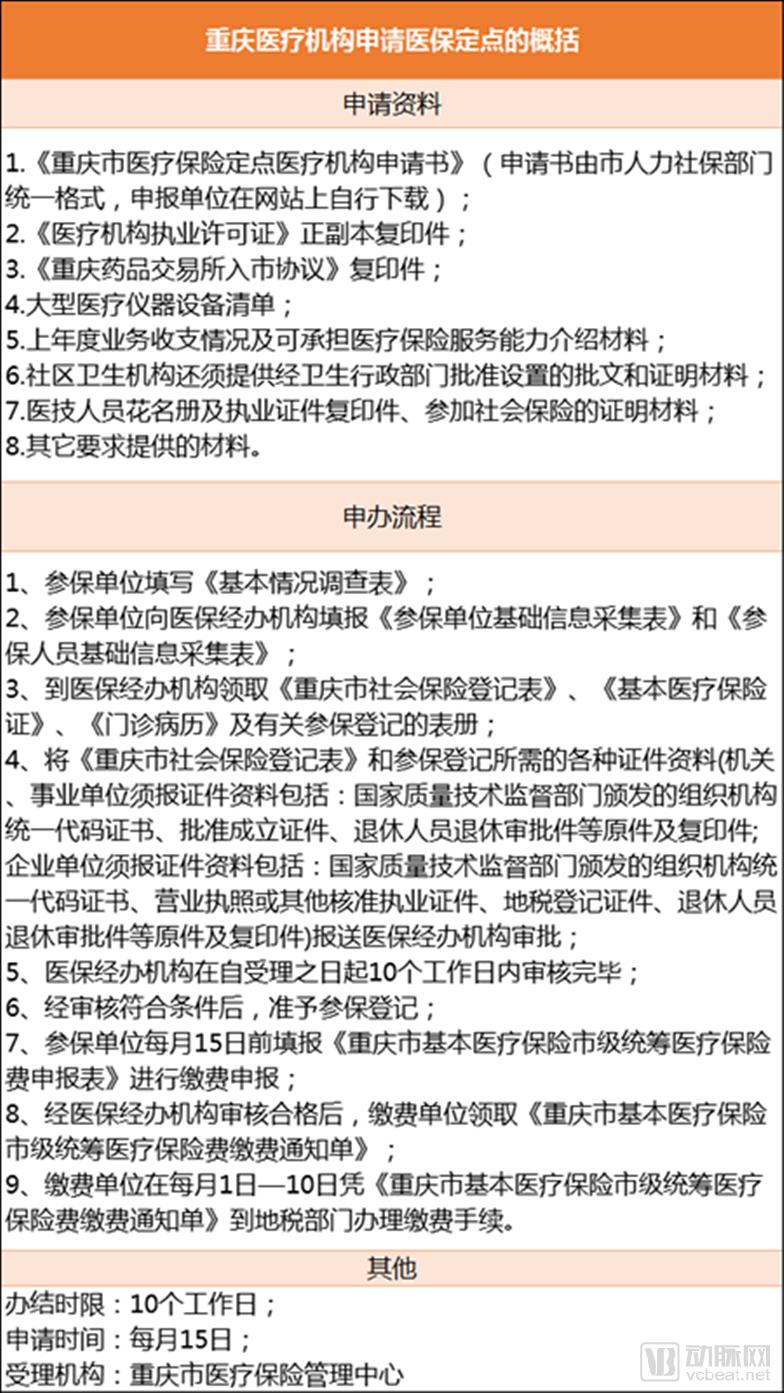
In short, there are four main steps for a clinic to enable medical insurance payment:
Check Policies: Review announcements on the local "Human Resources and Social Security Bureau" website, including detailed notices on timing, location, eligibility criteria, and required application materials.
Submit the application within 15 days. There is a window period for submission after the policy is released. Prepare the application materials as required by the announcement, including the "Application Form for Designated Medical Institutions under Basic Medical Insurance Agreement in XX City" and the "Self-Assessment Form for Designated Medical Institutions under Basic Medical Insurance Agreement in XX City."
The Medical Insurance Office working group conducts on-site reviews based on the submitted materials. Taking Hangzhou as an example, the overall activation process takes 6–9 months. While timelines vary by region, the general procedure remains similar; this information is for reference only, and the actual implementation difficulty depends on local administrative efficiency.
Although the scope of medical insurance payment agreements for clinics is limited to outpatient services, outpatient reimbursement under medical insurance is categorized into special outpatient and general outpatient care. Taking the Chengdu region as an example, the coverage for special outpatient reimbursement is primarily divided into the following categories:
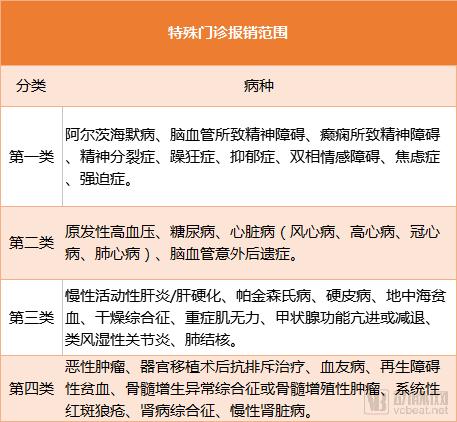
Special Outpatient Reimbursement Rate:Medical expenses incurred within a single treatment period that fall within the scope of diagnosis and treatment for special outpatient diseases shall be regarded as one-time inpatient medical expenses, and shall be reimbursed by the basic medical insurance pooling fund in accordance with the reimbursement standards for inpatient medical expenses.
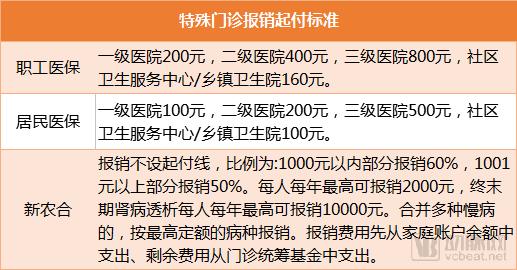
Conditions for Clinics to Apply for Special Outpatient Reimbursement: 1. Participation in Chengdu Medical Insurance in accordance with regulations; 2. Approval for special outpatient services has been obtained. Documents Required for Special Outpatient Reimbursement: Medical Insurance Card/Social Security Card, ID card, and other relevant materials. Process for Special Outpatient Reimbursement: Direct on-site settlement is available; insured individuals only need to pay their out-of-pocket portion, while the remaining costs are covered by the medical insurance fund.
In other words, once clinics are included in the special outpatient medical insurance payment system, they can attract more patients with chronic diseases. According to Li Changjiang, “Such special outpatient medical insurance coverage is currently available only at a few primary-level community hospitals or public community health service centers, primarily for hypertension and diabetes.” Since most of these patients seek treatment at tertiary Grade A hospitals, if clinics can stock the necessary medications and keep their diagnostic and therapeutic capabilities up to standard, it would be feasible for patients to return to primary care facilities for treatment and utilize medical insurance reimbursement.
In the future, once reimbursement for special outpatient services at clinics is enabled, it will help guide patients to seek medical care in an orderly manner and facilitate tiered diagnosis and treatment.
At this year’s Two Sessions, Ao Hushan, a member of the National Committee of the Chinese People’s Political Consultative Conference (CPPCC) and Chief Physician in the Department of Anesthesiology at Fuwai Hospital, Chinese Academy of Medical Sciences, stated that tiered diagnosis and treatment, as an institutional framework, encompasses the establishment of healthcare processes and systems such as initial consultations at primary care community facilities, tiered medical services, and two-way referrals. This system can address the difficulty of accessing medical care. Furthermore, medical fees under tiered diagnosis and treatment should be differentiated, with adjustments and guidance provided through health insurance payment mechanisms to genuinely reduce the financial burden of healthcare on the public. Its role is to ensure that medical institutions at all levels fulfill their respective responsibilities and leverage their unique advantages, thereby enabling residents to manage minor illnesses within their communities, ensuring orderly referrals for serious conditions, and normalizing health guidance, thus achieving the pro-public welfare objectives of healthcare reform policies.
Ao Hushan suggests that medical insurance plays a leveraged role in the tiered diagnosis and treatment system, and reforms should be explored in a timely manner. In accordance with the principle of “voluntary selection of nearby healthcare providers,” the guiding function of medical insurance settlement methods should be leveraged to encourage insured individuals to sign up for first-contact services with primary healthcare institutions. This approach aims to collaboratively advance the implementation of the first-contact physician responsibility system, the tiered consultation system, and the two-way referral system, while comprehensively implementing outpatient pooling. Notably, first-contact physicians are familiar with patients’ local customs and living environments, which is more conducive to the prevention and treatment of related diseases. As the number of patients with chronic diseases continues to rise in China, the effectiveness of the first-contact physician responsibility system in health management will become increasingly prominent. This strategy not only makes full use of healthcare resources at primary medical institutions but also effectively alleviates the patient intake pressure on central hospitals.
Meanwhile, outpatient pooling should be implemented based on the actual conditions of the basic medical insurance system. Outpatient pooling should be promoted in light of the essential healthcare needs of insured individuals, with reasonable determination of reimbursement rates, deductibles, and annual maximum payment limits under the outpatient pooling scheme. These parameters should be gradually increased as the fund’s financial capacity improves. Differentiated reimbursement ratios should be adopted to enhance the sustainability of the medical insurance system and maximize patient attraction to primary care institutions. Establishing a medical insurance payment system aligned with new models of community physician services constitutes the foundational driver for achieving tiered diagnosis and treatment. Medical insurance payment is not only a critical component of the revenue distribution mechanism for large medical institutions but also serves as the core incentive for actively promoting tiered diagnosis and treatment.
Certainly, in terms of management implementation, the establishment of a first-visit responsibility system and triage framework requires corresponding incentive and oversight mechanisms. At the operational level, healthcare security administration departments may provide performance-based bonus payments to primary care providers based on disease spectrum composition, patient age, and the service volume of first-contact physicians. Meanwhile, by refining health insurance reimbursement methods—such as increasing reimbursement rates and lowering deductibles for patients referred to tertiary hospitals through the first-contact physician—the sustained advancement of the first-visit system can be encouraged. Furthermore, the quality of referrals made by first-contact physicians can be monitored through assessment methods such as tracking patient health outcomes; physicians who fail to meet standards may be subject to regulatory interviews, public disclosure, or even penalties.
Furthermore, Ao Hushan suggested placing equal emphasis on the sustained training of general practitioners and encouraging outstanding university graduates to gain practical experience at the grassroots level, thereby enabling healthcare professionals to encounter a wider variety of cases and accumulate relevant expertise. To avoid blind referrals that may result from the mandatory use of essential medicines, and to prevent drug abuse stemming from inadequate triage supervision, primary care institutions should be permitted to stock and utilize medications outside the National Essential Medicines List. Additionally, he advocated for encouraging the development of private clinics and novel healthcare service models to promote an increase in high-quality medical resources.
“Using medical insurance as a lever to promote tiered diagnosis and treatment has inherent limitations. The medical insurance authorities and health departments should adopt a dual-pronged approach, and enforce implementation in coordination with multiple relevant departments to more effectively advance the tiered diagnosis and treatment system,” said Ao Hushan.