China Elevates EMR Evaluation Standard from Level 7 to Level 8, Driving Authentic Value Beyond Cosmetic Compliance
On March 23, the Chinese Hospital Information Network Conference (2018 CHINC) was held as scheduled at the Hangzhou International Expo Center.
“Digitalization, informatization, internet integration, and intelligentization”—these four terms set the keynote tone for this conference. While a relatively calm opening was anticipated, an unexpected bombshell dropped on the very first day: new standards are to be introduced for the graded evaluation of electronic medical records.Building on the previous maximum of seven levels, an eighth level with greater difficulty has been added.。
This change inevitably invites speculation: if the difficulty of electronic medical record (EMR) grading—long a persistent challenge for hospitals—is further increased, can it still reflect its original value?
This question has been clearly answered by several experts, including Associate Researcher Shu Ting from the Hospital Management Institute of the National Health and Family Planning Commission, Liu Haiyi, Director of the Information Management Department at Beijing Tsinghua Changgung Hospital, and Wang Tao, Director of the Information Center at Beijing Tiantan Hospital, Capital Medical University.
Differences Between the 2011 and 2018 Versions of the Electronic Medical Record (EMR) Grading Evaluation Method
In the current overall development of electronic medical records (EMR), Shu Ting presented a set of striking data: At present, EMR systems have been implemented in nearly 6,000 medical institutions at the secondary level and above, including 4,088 secondary hospitals, accounting for 52% of such hospitals nationwide, and 1,755 tertiary hospitals, representing 80% of their kind across China. The average application level in tertiary hospitals has increased from Level 1.58 to Level 2.11, while that in secondary hospitals has risen from Level 0.67 to Level 0.83.
In his interpretation of the “New Standards for Grading and Evaluation of Electronic Medical Records,” Liu Haiyi argued that the previous rating methodology—namely, the “Grading and Evaluation Methods and Standards (Trial) for Functional Application Levels of Electronic Medical Record Systems” issued by the General Office of the Ministry of Health in October 2011 (Document No. [2011] 137 of Wei Ban Yi Zheng Fa)—accomplished two revolutionary tasks. First, it established a method for evaluating the application level of electronic medical records; second, it designed approaches for both partial and comprehensive assessments.
Local assessment includes:
Specifies nine roles in the application workflow of electronic medical records;
37 specific assessment items were established;
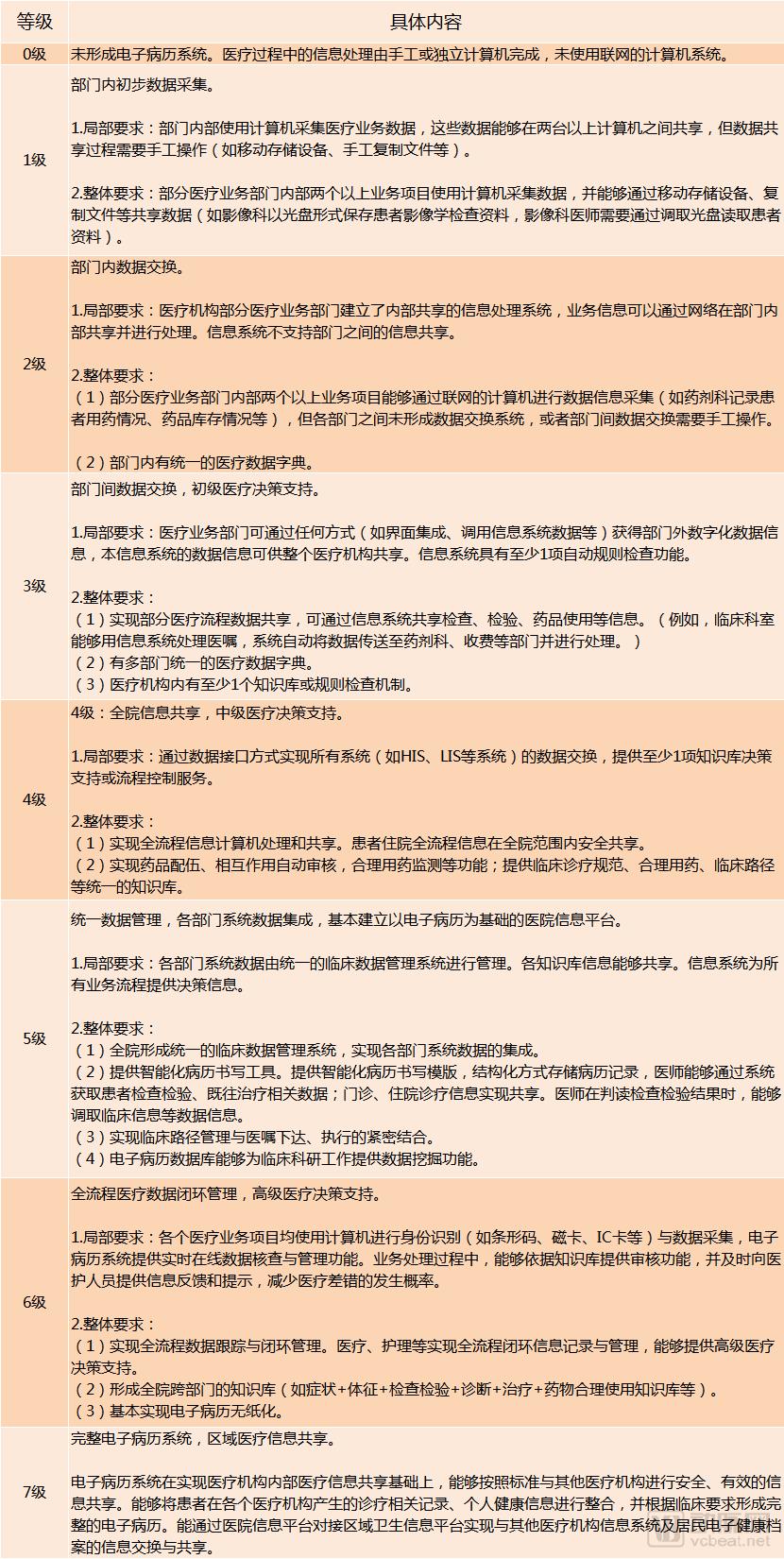
Propose level assessment requirements according to 8 levels (Level 0-7).
Overall assessment includes: comprehensive total score, and evaluation of selected items.
The evaluation model of the entire system is divided into three major levels, namely:
Level 1: Data Acquisition (data entry into computer systems); Level 2: Information Sharing (network data transmission and multi-departmental information sharing); Level 3: Intelligent Support (knowledge base support, comprehensive information assessment, and automated alerts).
The 2011 version of the quantitative scoring method for application levels is as follows:
Including:Ward Physicians, Ward Nurses, Outpatient Physicians, Diagnostic Departments, Laboratory Departments, Treatment Departments, Medical Insurance Support, Medical Record Management, FundamentalsA total of 9 standard medical roles.
Among the 37 specific evaluation items,There are 19 Level-4 basic items and 18 optional items.。
The achievements obtained in this phase are:
The overall average level of EMR application in hospitals has improved; after evaluation, hospitals have enhanced their capacity for planning the development of electronic medical record (EMR) systems; EMR software developers are focusing on information sharing and system functional integration, with particular improvements in interoperability with systems from other vendors.
This has given rise to five new major demands:
1. A large number of hospitals in China with low-level electronic medical record (EMR) applications require inclusion in the assessment.Discrimination;
2. Evaluate the scope of electronic medical records andIncomplete Coverage, there are new demands for medical quality control, knowledge base application, and data utilization, which currently guide the direction of applications;
3. Current Standard Evaluation ItemsContent Overlap;
4. Descriptions of Selected ProjectsInsufficiently clear, affecting comprehension during use;
5. Some hospitals blindly pursue higher accreditation levels, resulting in actualLow Data Quality。
To address these five major needs, the current electronic medical record (EMR) grading evaluation has been revised around six basic principles:
1. Maintain stability: Ensure that previous evaluations remain comparable to the greatest extent possible;
2. Enhance Discriminatory Power:Add a level and adjust the grading., migrate some functionalities into1-2 grades higherwithin the requirements;
3. Expand the scope of evaluation: Incorporate medical quality improvement initiatives into the assessment and add application roles;
4. Specify the content of examination, testing, and treatment items in the original evaluation function;
5. Add an evaluation dimension,Incorporate data quality (information quality) content into the assessment.. For different levels, list the assessment requirements for data quality;
6. Revise the content in the original instructions to avoid ambiguous statements.
Specifically manifested in:
The level of evaluation is based on past8 levels (levels 0-7) increased to 9 levels (levels 0-8), to enhance the discriminative power of low-grade assessments;
Adjust the difficulty levels to align with the current state of electronic medical record (EMR) system development in China.

Comparison of Implementation Difficulty Between the Old and New Versions
A comparison of the basic content between the old and new versions clearly reveals that, following the adjustment of standards,Overall, the implementation difficulty for Levels 1–4 has decreased, remains largely unchanged for Levels 5–6, and is relatively high for Levels 7–8.。
In addition, as previously mentioned, this evaluation also considers the assessment of information quality as a key factor in comprehensively evaluating the successful application of electronic medical record systems.
Contents include:
Data Standardization: Consistency between data records and dictionaries in the project;
Data Integrity: Completeness of data item content;
Data Integrity: Data items in related systems can be cross-referenced or linked;
Data Timeliness: Completeness and logical rationality of time-related items in the project (process time distribution)
Specifically reflected in:
Grades 0–2: No requirements;
Level 3: Focuses on assessing the consistency between key data items and dictionaries;
Level 4: Focus on the completeness of mandatory fields;
Level 5: Focuses on the completeness of mandatory and commonly used fields, with comprehensive data source mapping;
Level 6: Focuses on data integration and data timeliness;
Level 7: Focuses on assessing the comparability of data related to regional collaboration, as well as the completeness and timeliness of data content pertaining to medical quality management.
In terms of standard medical roles and items, the new evaluation method's roles build upon the original nine categoriesWard Physicians, Ward Nurses, Outpatient Physicians, Diagnostic Departments, Laboratory Departments, Treatment Departments, Medical Security, Medical Record Management, BasicsPosterior,AddedData UtilizationOne item, totaling 10 items.
Furthermore, the number of evaluation items in the new version has increased from 37 in the old version to 39. Among them, the 2011 version'sInpatient Medical Knowledge, Outpatient Medical Knowledge, and Access Control for Case DataThree items were canceled, and five new items were added:Clinical Data Integration, Medical Quality Control, Knowledge Acquisition and Management, Electronic Health Record Documentation Application, Infrastructure Security Management and Control. Notably, infrastructure security controls have been incorporated into the basic requirements, which means that in addition to the electronic medical record (EMR) software itself, its supporting hardware and network environment will also become factors in the assessment.
What Kind of Digital Signatures Meet Legal Requirements?
During the interpretation session of the “Specifications for the Application and Management of Electronic Medical Records (Trial),” Wang Tao primarily highlighted two major risks associated with existing digital signatures:
1. The specificity of signature content: Currently, no standards have been issued for the content of electronic medical record signatures. This leads to Certificate Authorities (CAs) not verifying whether the content being signed contains any issues during the signing process, thereby creating a risk that patient identities could be “swapped.”
2. Integrity of Signature Content. Due to the high frequency of hospital signatures, the Certificate Authority (CA) is unable to detect whether each submitted document contains adverse information during signature verification.
The aforementioned two risks can be mitigated through the use of signatures combined with timestamps. This approach ensures that the identity of the operator and the time of each operation are queryable and traceable.
Returning the Graded Evaluation of Electronic Medical Records to Its Essence
Based on the foregoing, we have drawn three core conclusions regarding the evaluation of the new version of electronic medical records (EMR) and its management specifications:
1. The tiered evaluation system has been expanded from eight to nine levels. This change does not merely increase difficulty as one might assume; in fact, the difficulty of lower-level assessments has been relatively reduced, mid-level difficulty remains unchanged, and higher-level difficulty has increased. As a result, the lowered threshold for lower tiers will inevitably lead to more hospitals passing accreditation at Level 4 and below, while stricter criteria have been imposed for hospitals seeking higher-level accreditation.
2. Data quality has become the focal point of accreditation, eliminating the possibility of hospitals passing reviews with falsified data as in the past and steering the evaluation process back to its essence—namely, the accumulation, sharing, and utilization of truly valuable big data.
3. Hospitals should exercise greater caution in selecting digital signature solutions and must ensure technical integrity to avoid potential legal loopholes and prevent unnecessary losses.
This indicates that the graded evaluation and application of electronic medical records (EMRs) are returning to their fundamental purpose, thereby enhancing the true value of EMRs rather than serving merely as a superficial showcase for hospitals.