Sparrow Health Leverages AI to Tackle Personalized Medicine Challenges: Empowering Oncologists with Adverse Reaction Prediction and Management
Currently, a surge of medical AI companies has emerged in China, with most focusing on image interpretation services for radiology and other diagnostic departments. Many of these enterprises offer products with limited functionality, resulting in significant homogenization.
However, as the core of hospitals, clinical departments are directly related to medical quality and patient health. Among these enterprises, companies that serve clinical departments are in the minority. Medbanks Network is one such innovative enterprise dedicated to serving oncology clinicians.
Artificial Intelligence Is the Foundation of Personalized Medicine
Personalized Medicine, also known as Precision Medicine: A customized healthcare model that designs optimal treatment plans tailored to individual patients based on their personalized information—including clinical data and various omics profiles—through medical decision-making, practices, and interventions, with the aim of maximizing therapeutic efficacy while minimizing adverse effects.
At present, personalized medicine or precision medicine has become a hotspot in the global medical community, and international pharmaceutical giants have long made personalized diagnosis and treatment their R&D focus.
Generally speaking, personalized medicine encompasses two aspects:
1. Personalized Diagnosis and Assessment: This primarily involves the integration of diverse information, relying on molecular diagnostic technologies, clinical big data, and cloud computing. Currently, as omics data at the molecular level remain incomplete, the enhanced utilization and mining of clinical data constitute a critical component of precision medicine. By collecting and analyzing data from individual patients, relevant diagnostic and assessment outcomes are derived. For complex cases requiring the integration of multiple factors, reliance on artificial intelligence technologies, such as data mining algorithms, is also essential.
Second, personalized treatment: Patients can receive individualized therapy based on risk assessment, achieving “tailored medication.”
According to Dr. Tao Ying, Chief Artificial Intelligence Officer of Medbanks Network Technology, the realization of personalized medicine requires the support of at least three factors:
1. Clinical Guidelines;
2. Individualized real-world patient data;
3. Artificial Intelligence Algorithms and Models.
Clinical guidelines provide fundamental decision-making references for personalized medicine. Currently, various countries, disciplines, and professional societies have published a wide array of disease treatment guidelines and consensus statements. These guidelines and consensus statements represent viewpoints and opinions formed based on existing research evidence regarding the treatment of specific diseases or the use of specific medications, aiming to guide the clinical practice of general physicians.
Clinical guidelines typically target a broad patient population and are generally generalized in nature. Due to individual variations among patients, these guidelines cannot provide a definitive, personalized treatment plan that covers all cases. Certain less common scenarios are often inadequately addressed, such as elderly patients presenting with multiple comorbidities.
Currently, in most cases, physicians must rely on their clinical experience to make judgments and provide personalized treatment for patients not covered by clinical guidelines. However, this approach presents numerous challenges, including insufficient physician experience and the considerable difficulty humans face in accurately and scientifically calculating risk probabilities by integrating multiple factors.
In this context, leveraging real-world patient data to construct mathematical models via machine learning and other algorithms, conducting risk assessments for patients using these models, and ultimately informing clinical decision-making has become a key direction in supporting physicians with personalized medicine.
How to Build a Personalized Prediction Model?
According to Dr. Tao, Medbanks Network Technology is developing a risk prediction system for adverse reactions caused by tumor chemotherapy, codenamed “Sherlock Holmes.” Dr. Tao also stated that the establishment of personalized prediction models requires the following steps:
First, it is necessary to define the prediction objectives and the specific medical problems to be addressed. Subsequently, based on these prediction goals, individual real-world patient data should be collected, rather than aggregate statistical data. To date, Medbanks Network Technology has established an oncology database comprising approximately 450,000 patient records. These data are sourced from more than 700 oncology-related departments across over 300 hospitals.
Once the database is established, the next step involves data cleaning and modeling. This includes selecting appropriate data algorithms and iteratively optimizing model parameters to achieve optimal predictive performance, such as maximizing the area under the receiver operating characteristic curve (AUC).
Taking Medbanks’ chemotherapy-induced nausea and vomiting (CINV) prediction model as an example, the underlying database comprises 12,000 lung cancer patients and 23,292 cycles of systemic therapy, collected from 19 oncology-related departments across 12 provinces. Through multiple rounds of testing, the Naive Bayes algorithm, demonstrating the strongest generalization capability and robustness, was ultimately selected for statistical analysis.
This algorithm can provide a relatively accurate risk probability, enabling physicians to develop personalized prophylactic regimens for chemotherapy-induced nausea and vomiting (CINV) by integrating this probability with clinical guidelines.
For instance, patients with a risk greater than 90% should be administered three antiemetic agents, those with a risk less than 10% may not require pharmacological intervention, and those with intermediate risk may receive one or two agents. Such personalized management maximizes the prevention of adverse reactions while avoiding overtreatment.
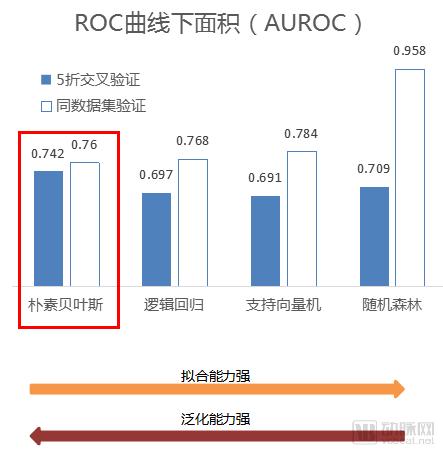
Model Evaluation: For binary classification problems, the most commonly used method is the area under the ROC curve, which is plotted with the true positive rate (sensitivity) on the y-axis and the false positive rate (1-specificity) on the x-axis.
Generally, the area under the ROC curve (AUC) ranges between 0.5 and 1.0. When AUC > 0.5, the closer the AUC is to 1, the better the diagnostic performance. An AUC of 0.5–0.7 indicates low accuracy; an AUC of 0.7–0.9 suggests moderate accuracy; and an AUC above 0.9 reflects high accuracy. An AUC of 0.5 implies that the diagnostic method has no discriminatory power and lacks diagnostic value. An AUC < 0.5 is inconsistent with reality and rarely occurs in practice.
After the initial model is developed, it must be validated in real-world hospital settings to finalize the model. During this process, the model may still encounter issues such as overfitting. Benefiting from a large dataset, Medbanks’ chemotherapy-induced nausea and vomiting (CINV) prediction model has achieved an AUC of 0.87 in actual hospital validations, representing a high level within the industry.
See the figure below:
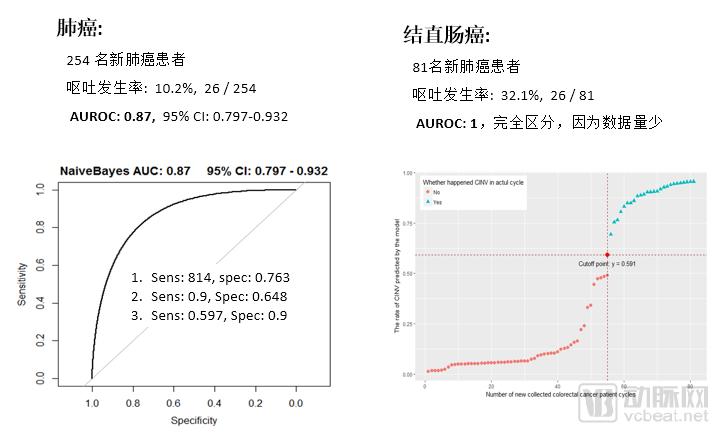
Due to the limited number of cases for certain tumors, Medbanks primarily designs models for major cancer types, such as lung cancer and colorectal cancer. It is reported that, in addition to modeling chemotherapy-induced nausea and vomiting (CINV), Medbanks is developing a predictive model for chemotherapy-induced myelosuppression, which is of greater significance to both physicians and patients. The model has yielded promising preliminary results and awaits further validation in clinical settings.
Medbanks’ decision-support tools are primarily developed and validated through its WeChat Official Account and mobile app. Currently, the WeChat Official Account platform is being used by more than 1,000 physicians. Any user of the Medbanks Oncology Database can activate the app-based product, which effectively provides physicians with access to a “mobile database.”

Can AI Products Be Used in Clinical Practice?
Can Artificial Intelligence Be Applied to Personalized Medicine in Clinical Departments at the Current Stage? The Most Authoritative Voices Come from Clinicians. In this regard, VCBeat interviewed two oncology experts from top-tier hospitals in China, hoping to obtain answers to this question from them.
According to Cui Chuanliang, Associate Chief Physician in the Department of Renal Cancer and Melanoma at Peking University Cancer Hospital, current cancer treatments are primarily categorized into three major types: immunotherapy, targeted therapy, and conventional chemotherapy.
When selecting a treatment regimen, physicians first determine the overarching therapeutic strategy, deciding whether to use immunotherapy agents, targeted therapies, or conventional chemotherapy. Once the direction is established, they select specific medications based on the patient’s organ function, sites of metastasis, and the adverse effect profiles of the drugs.
In this process, clinical guidelines serve to guide the broad selection of therapeutic modalities, such as determining which patient populations are suitable for immunotherapy, targeted therapy, or chemotherapy. Physicians then integrate individualized patient parameters—including specific mutation sites, molecular targets, organ function status, and the presence of contraindications—to ultimately determine the specific drug or treatment modality, dosage, and duration of therapy.
On this point, Dr. Zheng Yulong, Associate Chief Physician in the Department of Medical Oncology at The First Affiliated Hospital, Zhejiang University School of Medicine, provided the same answer. He believes that clinical guidelines serve only as a reference for physicians in cancer treatment; specific therapeutic approaches should be personalized based on individual patient data, such as liver and kidney function and genetic profiles.
According to VCBeat, the indications for a drug are generally determined based on the level of evidence. If a drug has a high level of evidence supporting its use in a specific patient population, physicians need only administer it to patients at the recommended dosage and duration. Generally, the higher the level of evidence, the more likely it is to be included in the drug’s package insert.
For this reason, the package insert typically provides only the recommended dosage and range for a drug. However, the therapeutic scope of many drugs is often broader, with numerous indications not included in the labeling. Physicians may prescribe a drug for a specific disease only when there is clear evidence from randomized controlled trials (RCTs) supporting its use.
Once adverse reactions occur in patients during tumor treatment, physicians will implement different management strategies based on the severity of the toxicity. Generally, mild (Grade 1) and moderate (Grade 2) adverse reactions can be managed with continued observation. For severe adverse reactions, such as severe (Grade 3) or potentially life-threatening (Grade 4) events, treatment discontinuation or dose reduction will be implemented.
“Typically, our treatment protocols involve premedication; for instance, we prescribe prophylactic antiemetics based on the patient’s clinical condition and financial status,” said Director Cui.
Due to limited experience with adverse reactions, some physicians are likely to overlook rare adverse events or misattribute them to other causes.
In response, Director Zheng stated, “If artificial intelligence systems can provide alerts for rare adverse reactions, it will enable clinicians to more comprehensively consider patients’ medication and treatment regimens.”
Regarding the application of artificial intelligence products in personalized diagnosis and treatment, the two directors offered profound insights:
Director Zheng believes that AI products must accurately reflect patients’ real-world conditions, making model accuracy and data authenticity critical. Given the current fragmentation of hospital data, relying solely on clinical course records is insufficient to fully capture a patient’s specific situation; incorporating follow-up and genomic data is essential to ensure credible results.
Director Cui believes that AI models similar to those developed by Medbanks are currently more suitable for routine patient treatment, helping to ensure that physicians avoid significant errors in diagnosis and therapy. However, for diseases with few reported cases, the limited sample size makes it difficult for clinicians to draw conclusions based on model predictions alone; therefore, such applications may not yet be appropriate for these scenarios. Consequently, companies could begin by closely observing a defined patient cohort to test whether their models can accurately predict drug efficacy and adverse reactions.
Hospitals, Physicians, Pharmaceutical Companies, and Patients All Benefit
According to Tao Ying, Medbanks’ AI products primarily serve hospitals and pharmaceutical companies, with patients being the ultimate beneficiaries.
The hospital’s need lies in assisting physicians with diagnostic and therapeutic decision-making based on risk prediction criteria, helping healthcare professionals prevent and manage adverse reactions in patients during chemotherapy and pharmacotherapy, thereby reducing unnecessary medication use or omissions.
For pharmaceutical companies, a higher incidence of adverse drug reactions is detrimental to market promotion. Medbanks’ AI-powered solutions enable earlier detection, reporting, and reduction of adverse drug reaction events.
Furthermore, the use of artificial intelligence can enhance patient medication adherence. For instance, based on risk predictions, physicians can proactively prescribe antiemetic medications to patients before the onset of nausea and vomiting, thereby reducing the likelihood of treatment discontinuation and ensuring therapeutic efficacy.
Furthermore, Medbanks’ predictive models can also be used to identify contraindications for new drugs. By analyzing model outputs, the system alerts pharmaceutical companies to patient populations at higher risk of adverse reactions, thereby facilitating updates to their product labeling and package inserts.
For every hospital department it partners with, Medbanks dispatches data entry clerks to assist physicians in collecting and organizing data. All patient data obtained by Medbanks undergoes de-identification by the hospitals, ensuring that no sensitive patient information is included.
Tao Ying revealed to VCBeat that Medbanks has positioned its focus on oncology-related departments, rather than the currently popular imaging or pathology departments, because the company believes that clinical departments are the core of hospitals and is optimistic about the application of artificial intelligence in clinical settings.