Restructuring Healthcare Production Relations: Unlocking New Commercial Opportunities — Business Value Report on Medical Consortiums
The restructuring of the industrial ecosystem will inevitably bring about business opportunities.
Traditional healthcare institutions are delineated by geographic location. The Medical Consortium, leveraging advanced information technology, redefines the boundaries of these traditional entities. Within a given region, multiple healthcare institutions are integrated into functional departments of the Consortium based on their respective capabilities and strengths, through functional division and labor redistribution. Consequently, the Medical Consortium emerges as a larger, unified healthcare entity, where geographic constraints are diminished and the boundaries of traditional healthcare institutions are fundamentally redefined.
Compared with earlier forms of medical collaboration, Medical Alliances represent not merely technical cooperation, academic and talent exchanges, or paired assistance, but rather a unified integration in terms of management and accountability. In this model, healthcare institutions at all levels form collaborative alliances or medical groups, becoming communities of shared interests and responsibilities.
In the traditional healthcare service system, patients and insurers are the ultimate payers in the medical industry chain, which is an ecosystem centered on physical medical institutions. Both upstream suppliers and downstream payers revolve around these medical institutions as the core.
Therefore, the profound transformation within healthcare institutions themselves, particularly the significant changes in their internal relationships, will inevitably impact external suppliers, payers, and various service providers. Formally speaking, the Medical Consortium policy redefines the business relationships among healthcare institutions. From a commercial perspective, the reform of healthcare institutions into Medical Consortia will inevitably lead to the disintegration of the traditional healthcare commercial chain. For market participants, this shift conceals substantial changes and risks, while also harboring significant business opportunities.
How Are Medical Consortia Reshaping the Healthcare Ecosystem? What Commercial Value Do They Bring? Starting from the perspective of healthcare resource flow, this report explores the essence of medical consortium reform and provides an in-depth analysis of the future business opportunities and new healthcare ecosystem brought about by medical consortia, thereby supporting corporate strategic upgrades.
This report comprises 65 pages, 39 charts and graphs, and a total of 25,000 words. The table of contents is as follows:
Chapter 1: Medical Consortia Reconstruct Healthcare Production Relations, Comprehensively Enhancing Resource Value
1, The Rigidity and Imbalance of Medical Resources Hinder the Enhancement of China's Healthcare Service Capacity
2. Tackling Industry Challenges, Establishing Resource Circulation Mechanisms, and Policy-Guided Comprehensive Promotion of Medical Consortiums
3. With over 5,000 entities, medical consortiums deliver tangible operational effectiveness
4. Six Dimensions: Analyzing Differences Among Various Types of Medical Consortiums
5. Management issues are the biggest obstacle to the implementation of medical consortia; currently, the service capacity of primary healthcare institutions is not the main factor affecting their implementation.
Chapter 2: Medical Consortiums Reshape the Healthcare Ecosystem, Creating New Commercial Entry Points
Chapter 3: Healthcare Informatics—Building the Technological Foundation for Medical Consortiums
1. The urgent need for IT solutions in the construction of medical consortiums brings significant industry benefits
2. Establishing an Independent Information Service Platform to Serve the Medical Consortium
3. Low levels of electronic medical record (EMR) adoption in county-level hospitals hinder business interoperability within medical consortiums
4. WeDoctor: Centered on “WeDoctor Cloud,” it builds an internet healthcare ecosystem and promotes the implementation of medical consortia.
5. Xinyi International: Building Core Competitiveness and Empowering Physical Healthcare Through “Technology + Resources + Operations”
Chapter 4: Medical Consortiums Drive the Implementation of Pharmaceutical Distribution Reform, ushering in Major Industry Changes
1. Anhui’s “16+1” Medical Consortium Volume-Based Procurement with Price Caps Reflects the Trend of Transformation in Pharmaceutical Distribution Channels
2. Decentralization of Chronic Disease Management and Standardization of the Drug Formulary Drive Growth in Primary Care Medication Use
3. Mingyi Zhonghe: Building a Medical Consortium and Pharmaceutical Service Platform by Starting with Grassroots Informatics
Chapter 5: Third-Party Medical Institutions Drive the Upgrading of Primary Care Services and Promote the Deepening of Primary Care Division of Labor
1. Iteration of Primary Healthcare and Ecosystem Restructuring Create Business Opportunities for Third-Party Independent Medical Institutions
2. Leverage third-party medical institutions as a nexus to establish multi-dimensional connections and empower primary healthcare
3. Tongxin Medical Alliance: A Closed-Loop Business Model Integrating Offline Imaging Centers with an Online Imaging Cloud Platform
The following is an excerpt from the report “Restructuring Healthcare Production Relations to Unlock New Business Opportunities: A Report on the Commercial Value of Medical Consortia.” For the full report, please refer to the download link provided at the end of this article.
Regional Medical Consortium, abbreviated as "Medical Consortium," primarily refers to the optimized integration of large and medium-sized medical institutions at different levels, with varying natures or management systems and affiliations, along with primary healthcare institutions within the same region under a relatively unified management framework. By implementing a group-based model, it establishes a standardized and regulated service pattern, aiming to achieve an integrated full-process service system encompassing preventive care, health services, and medical treatment.
Traditional healthcare institutions are delineated by geographic boundaries, whereas medical consortia redefine the boundaries of traditional healthcare institutions based on advanced information technology.
Medical alliances integrate multiple healthcare institutions within a specific region into internal functional departments based on their respective capabilities and strengths, through the division of functions and reallocation of responsibilities. Consequently, the medical alliance itself becomes a larger healthcare entity, where geographical influence is diminished and the boundaries of traditional healthcare institutions are redefined. Compared with earlier forms of medical cooperation, medical alliances represent not merely technical collaboration, academic and talent exchanges, or paired assistance, but rather a unified integration in terms of management and accountability. Healthcare institutions at all levels form collaborative alliances or medical groups, becoming communities of shared interests and shared responsibilities.
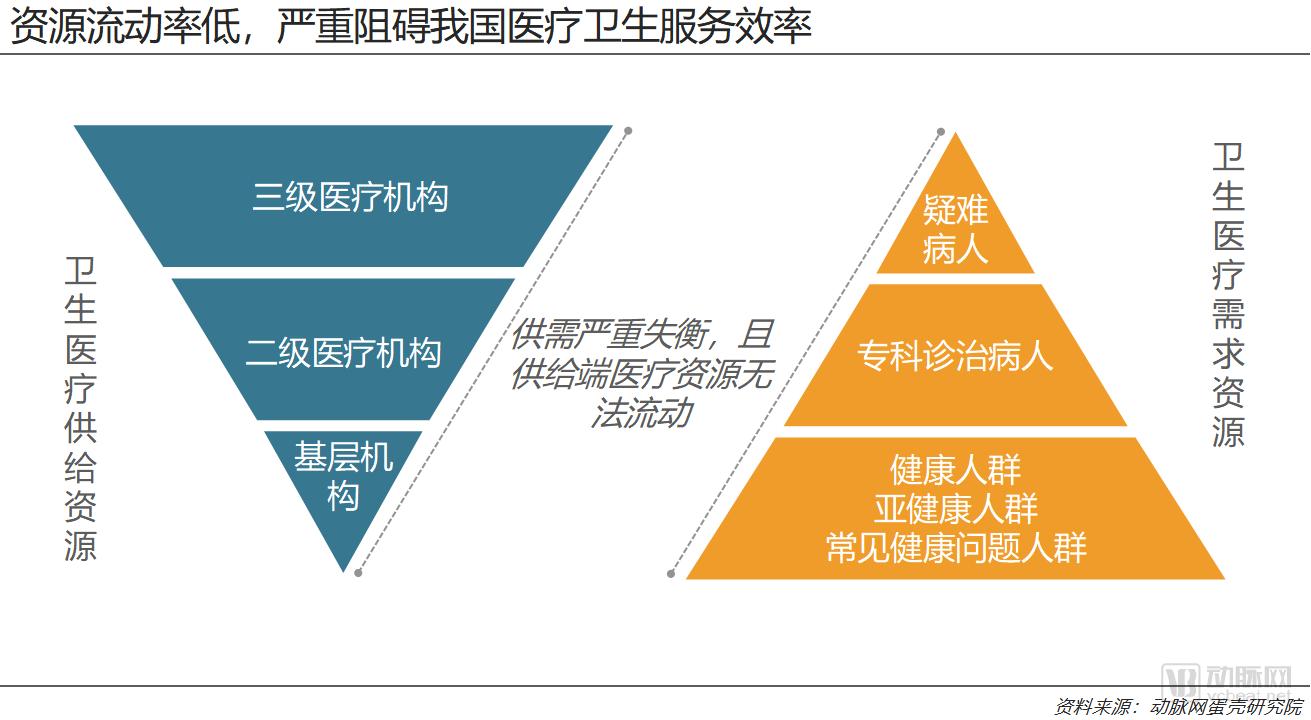
1. The Rigidity and Imbalance of Medical Resources Hinder the Improvement of China's Healthcare Service Capacity
Healthcare delivery is a production process that transforms medical resources into service outputs. Medical resources refer to the collective term for the factors of production involved in providing healthcare services, typically including personnel, medical expenditures, healthcare institutions, hospital beds, medical facilities and equipment, knowledge and skills, and information.
The rationality of resource allocation has a profound impact on the production efficiency of a system, and there is a clear correlation between resource mobility and the rationality of such allocation. Generally speaking, higher resource mobility facilitates more rational resource allocation, whereas lower mobility, or greater rigidity, often leads to less optimal allocation. Therefore, resource mobility is a key characteristic of modern economies and serves as an important indicator for assessing the quality and maturity of an economic mechanism.
A market economy is a crucial mechanism for achieving optimal resource allocation. A low degree of marketization indicates a lack of self-regulating mechanisms to ensure the rationality of resource allocation, resulting in low resource mobility and utilization rates, which leaves substantial room for efficiency improvements within the industry.
The healthcare industry is characterized by a relatively low degree of marketization, which is closely related to its positioning within the national economy. While public ownership facilitates state regulation of the sector and ensures basic medical security, the limited marketization prevents the self-regulating mechanisms of a market economy from functioning effectively. Consequently, China faces structural imbalances in the distribution of medical resources, which adversely affects the efficiency of healthcare services.
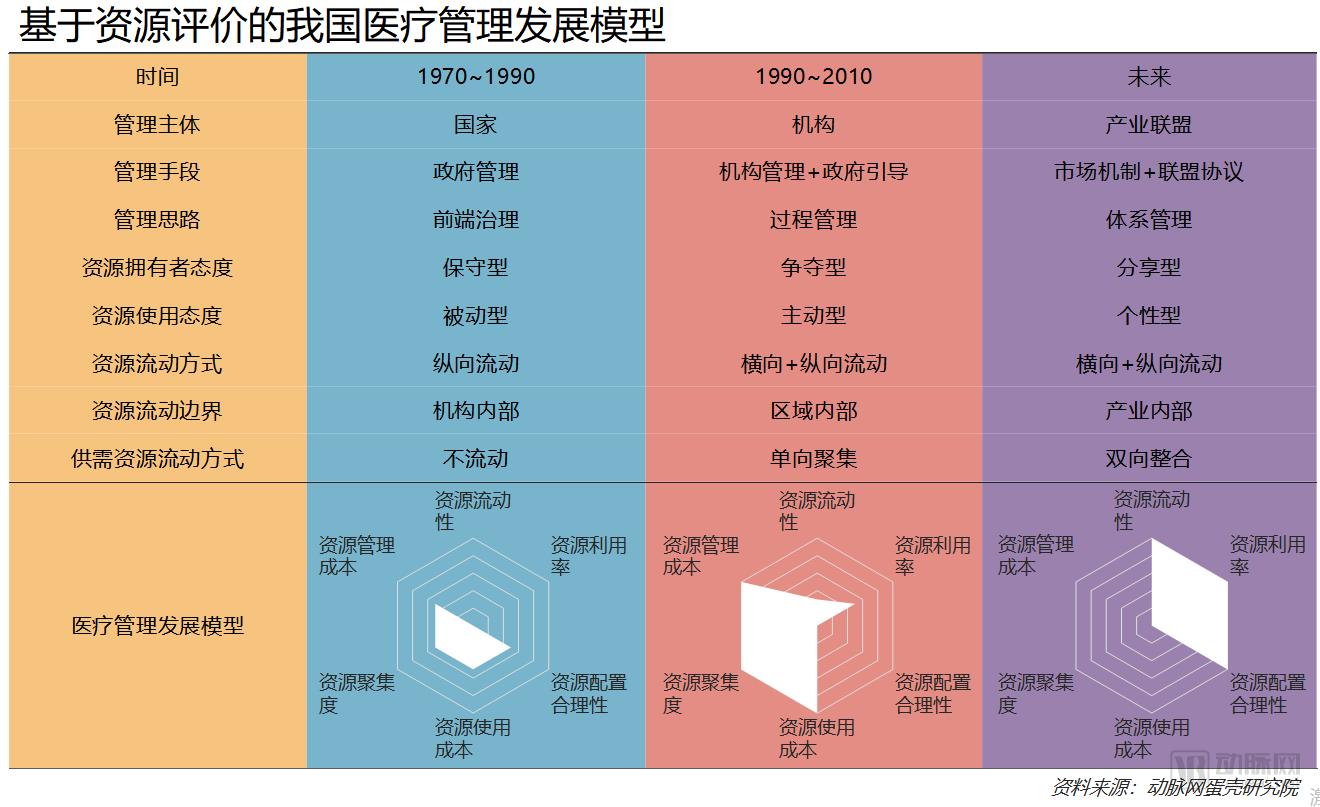
The development of medical management in China can be defined as three processes. From the perspective of resources, we conduct a model-based evaluation of the medical management system at different stages in China. Among them, resource evaluation includes six major indicators: resource mobility, resource utilization rate, rationality of resource allocation, resource management cost, resource usage cost, and resource concentration.
Since the 1990s, social factors such as consumption upgrading, demographic shifts, and environmental changes have driven a substantial increase in domestic healthcare demand. However, China’s healthcare service system is predominantly public-owned. The low mobility of medical resources has led to reduced utilization rates and suboptimal allocation, while significantly increasing resource management costs, concentration levels, and usage costs. This current state of resource utilization has greatly hindered the further enhancement of China’s healthcare service capacity.
If the current stagnation of medical resources cannot be improved, the rapid growth in healthcare demand driven by factors such as population aging and consumption upgrading will further reduce the service efficiency of the healthcare system. Addressing this challenge requires fundamental reforms in healthcare management, revitalizing medical resources, and achieving their optimized allocation. By enhancing resource utilization efficiency, we can strengthen the service capacity of China’s healthcare system.
The future healthcare management model features industrial alliances as the primary governing entities, achieving front-end governance of the healthcare system through a combination of market mechanisms and alliance agreements. Government functions will shift from initial front-end governance to systemic oversight. For healthcare resources, mobility will increase significantly. Due to changes in competitive dynamics, the boundaries of resource flow will expand from within individual institutions to across the entire industry, thereby substantially improving the rationality of resource allocation and utilization efficiency.
At the macro level, the integration of resources has enabled previously unidirectional and centralized medical resources—specifically, healthcare supply resources—to become mobile. Patient autonomy has been strengthened, gradually achieving bidirectional integration of supply and demand resources and enabling autonomous, rational allocation of resources.
Overall, driven by market mechanisms and alliance agreements, government administrative costs have decreased significantly, while the rationality of resource allocation has been substantially improved due to enhanced resource mobility. Through the restructuring of medical production relations, the industry has evolved into a collaborative landscape characterized by resource sharing and specialized division of labor. Satisfaction among doctors, patients, and the government has risen markedly, leading to significant improvements in the efficiency and value of medical services.
2. Addressing Industry Challenges, Establishing Resource Circulation Mechanisms, and Policy-Guided Comprehensive Promotion of Medical Consortia
The essence of tiered diagnosis and treatment is to integrate the entry points for healthcare service demand. By directing minor illnesses to primary care facilities and major illnesses to hospitals, this model enables healthcare institutions at all levels to better fulfill their respective roles, thereby improving the overall efficiency of the healthcare system. The “Medical Consortium” serves as a key mechanism for implementing the tiered diagnosis and treatment system. While establishing institutional linkages, Medical Consortia clarify the functional positioning of healthcare institutions at different levels, facilitate division of labor and collaboration among them, promote orderly patient access to care, and optimize the distribution of resources within the healthcare service system. This approach can significantly address the inefficiencies in China’s healthcare service system caused by structural imbalances in resource allocation.
Medical Consortiums: An Institutional Approach to Empowering Primary HealthcareThe purpose of establishing medical consortiums is to break down vertical and horizontal barriers among healthcare institutions, establish mechanisms for the circulation of medical resources, and optimize their allocation. As a result, primary healthcare institutions, which are typically resource-disadvantaged, can naturally enhance their service delivery capabilities.
Medical alliances represent an innovation in the traditional healthcare service system. By establishing and developing medical alliances, we can fully leverage the leading role of tertiary public hospitals within the region, guide medical institutions at different levels and of different categories to establish collaborative relationships with clear objectives and well-defined responsibilities, and promote the decentralization of high-quality medical resources. This approach can gradually address issues such as incomplete layout of the existing healthcare service system, insufficient supply of high-quality medical resources, and irrational allocation, thereby facilitating the formation of a tiered diagnosis and treatment system and encouraging patients to seek initial consultations at primary care facilities and receive medical services closer to home.
The Essence of Medical Consortia: Vertical Integration of High-Quality Medical ResourcesThe core of a medical consortium lies in connectivity. By leveraging the development of medical consortia as a breakthrough point, barriers between institutions at various levels—such as those related to fiscal investment, health insurance reimbursement, and personnel management—can be gradually dismantled, thereby fostering synergistic efforts in resource sharing and operational collaboration.
The core of medical consortiums lies in connectivity, with their essence being the establishment of a mechanism for the circulation of medical resources across different institutions. This facilitates both horizontal and vertical flow of resources, thereby promoting optimized resource allocation, enabling healthcare institutions to develop new operational logics and production relationships, and ultimately enhancing the overall efficiency of China’s healthcare service system.
From this perspective, the value of medical consortia to the future healthcare ecosystem is self-evident, and it is only natural for the government to serve as the core driving force behind their development.
In August 2016, the National Health and Family Planning Commission (NHFPC), later renamed the National Health Commission (NHC), highlighted in its “Notice on Advancing Pilot Programs for Tiered Diagnosis and Treatment” the exploration of establishing medical consortia. It stipulated that provincial and pilot city health and family planning administrative departments should engage in comprehensive planning to gradually form a regional collaborative service model with clearly defined responsibilities, authority, and benefits. By leveraging informatization tools such as telemedicine, these efforts aim to promote the sharing and vertical flow of regional medical resources, thereby improving the tiered diagnosis and treatment service system. Building upon existing initiatives, entities within the same region are encouraged to form medical consortia based on the principles of proximity and voluntariness, while avoiding cross-provincial structures. Furthermore, mechanisms for responsibility sharing and benefit distribution should be established within medical consortia to fully mobilize the enthusiasm of member institutions.
As can be seen from the notice, the government was very cautious in promoting medical consortiums at that time, which was specifically reflected in the phrases “pilot cities,” “exploratory establishment,” encouraging formation based on the principles of “proximity and voluntariness,” and “avoiding cross-provincial establishment.” The policy’s fundamental stance toward medical consortiums was to conduct exploratory establishment within limited regions in accordance with the principles of voluntariness and proximity.
It is particularly important to note that the policy also clarifies that medical consortia are a crucial component of tiered diagnosis and treatment; both “enhancing primary care service capacity” and “separate management of acute and chronic conditions” must be implemented with medical consortia as the vehicle.
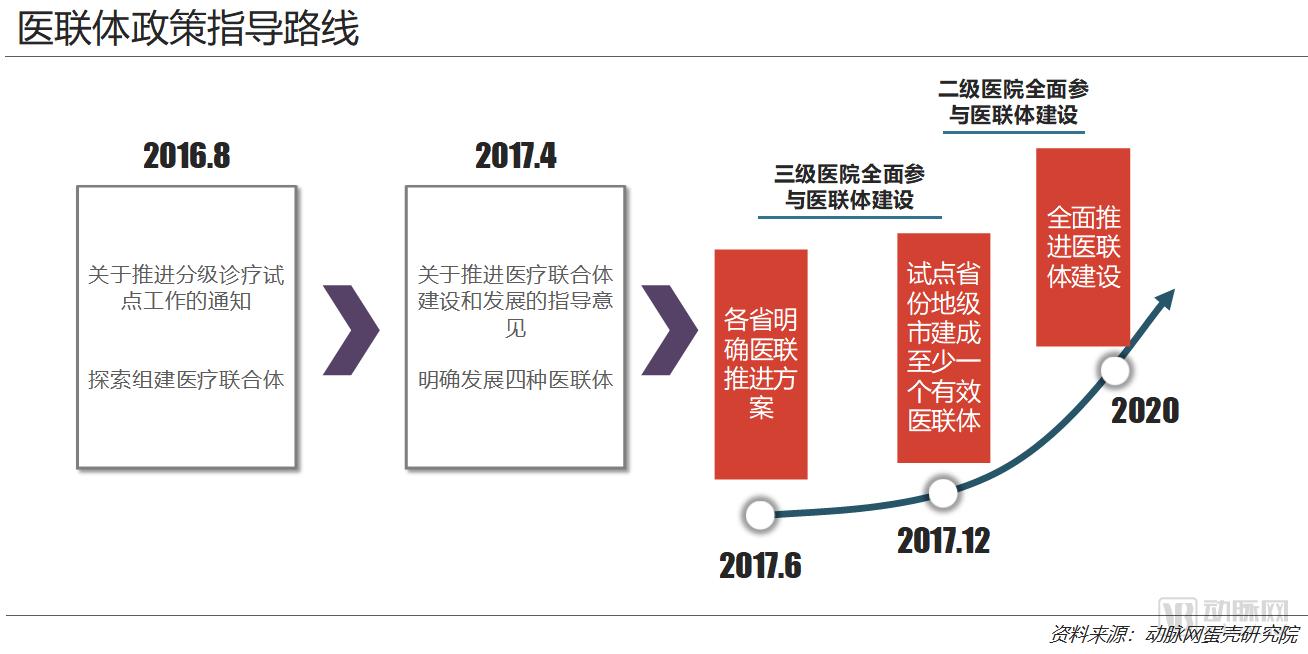
On April 12, 2017, the State Council executive meeting reviewed and approved the Guiding Opinions on Strengthening the Construction and Development of Medical Consortia. On the 23rd of the same month, the General Office of the State Council issued the Guiding Opinions of the General Office of the State Council on Promoting the Construction and Development of Medical Consortia. This document serves as a programmatic guideline for the comprehensive development of medical consortia, outlining not only the roadmap for their growth but also clarifying the key requirements for their establishment.
In contrast to the exploratory establishment of medical consortia in pilot cities under the “Notice on Advancing Pilot Programs for Tiered Diagnosis and Treatment,” this policy marked the commencement of comprehensive development of medical consortia and set forth specific implementation targets: “By the end of June 2017, all provinces (autonomous regions and municipalities) shall formulate work plans for advancing the development of medical consortia, specifying local objectives and timelines; by the end of October, all tertiary public hospitals shall initiate the development of medical consortia.” “By 2020, building upon lessons learned from pilot programs, the development of medical consortia shall be fully advanced nationwide, resulting in a relatively complete policy framework. All secondary public hospitals and government-run primary healthcare institutions shall participate in medical consortia.”
This includes two key milestone events: by the end of 2017, all tertiary public hospitals were required to initiate medical consortium operations; by 2020, all secondary public hospitals and government-run primary healthcare institutions were to fully participate in medical consortia.
In addition to advancing its objectives, the policy explicitly defines for the first time the four models of medical consortiums to be promoted in China:
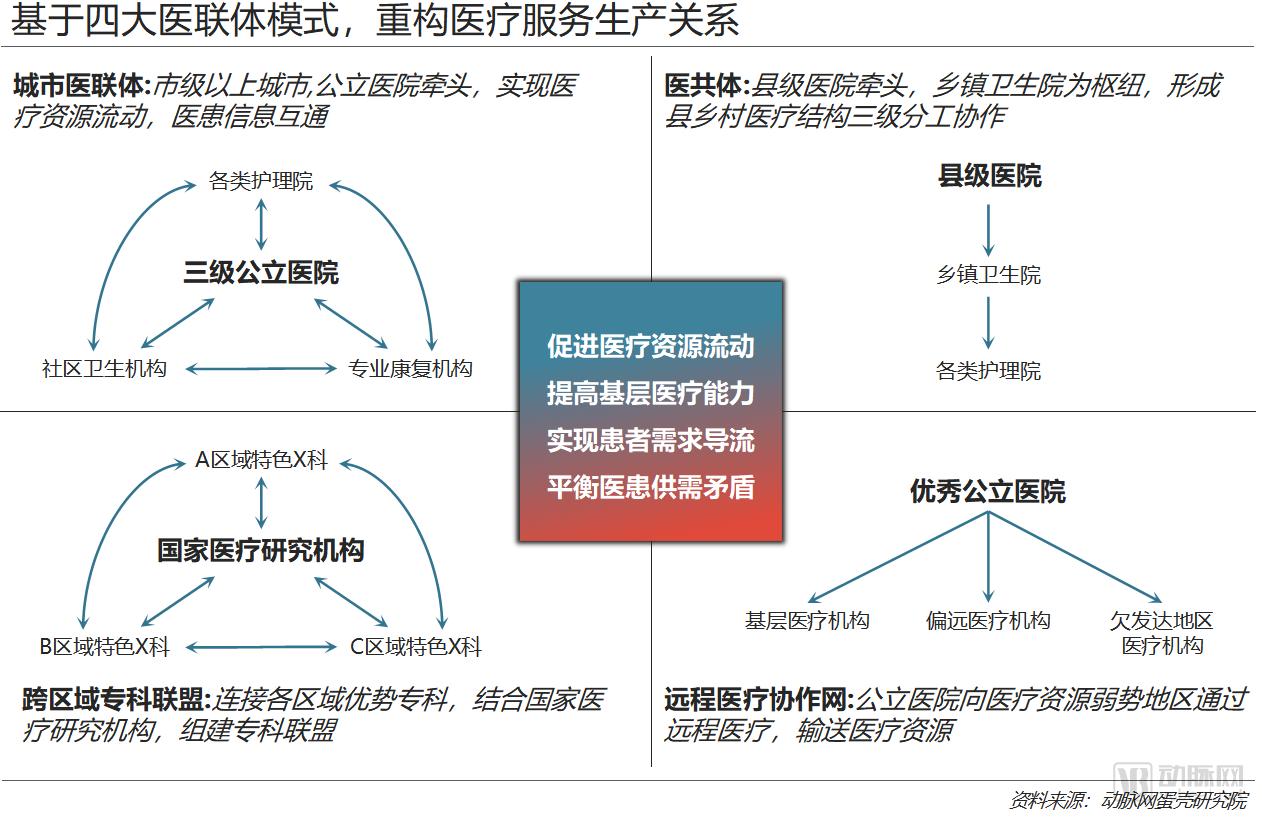
Urban Medical Group Model, urban medical consortiums (i.e., healthcare alliances) are categorized into two types: tightly integrated and loosely affiliated. Led by tertiary hospitals, these “1+X” medical consortiums bring together secondary urban hospitals, rehabilitation hospitals, nursing homes, and community health service centers to vertically integrate healthcare resources, thereby establishing a management model characterized by resource sharing and collaborative division of labor.
County-Level Medical Community Model, the county-level medical community is an integrated county-township management model led by county-level hospitals, with township health centers as hubs and village clinics as the foundation. It effectively interfaces with rural integration to establish a mechanism for division of labor and collaboration among three-tier medical and health institutions at the county, township, and village levels.
Specialized Medical ConsortiumA consortium formed among medical institutions through specialty collaboration, centered on the distinctive specialties of one institution and integrating specialized expertise from other institutions, establishes several regional centers of excellence. This model enhances the capacity to manage major specialty-specific diseases and fosters a complementary development pattern.
Telemedicine Collaboration Network, public hospitals provide telemedicine, remote teaching, and remote training services to grassroots, remote, and underdeveloped areas, leveraging information technology to promote the vertical flow of resources, enhance the accessibility of high-quality medical resources, and improve the overall efficiency of healthcare services.
Local Policies Follow Suit, with Goals Converging via Different Paths
Using “medical consortium/medical alliance” as keywords, VCBeat Research Institute conducted a search in the VCBeat policy database. We found that prior to 2017, although the term “medical consortium” appeared in the content of many other policies, very few policies issued by either the national or local governments included “medical consortium” in their titles. In 2017, the number of such policies surged from 9 in 2016 to 51.
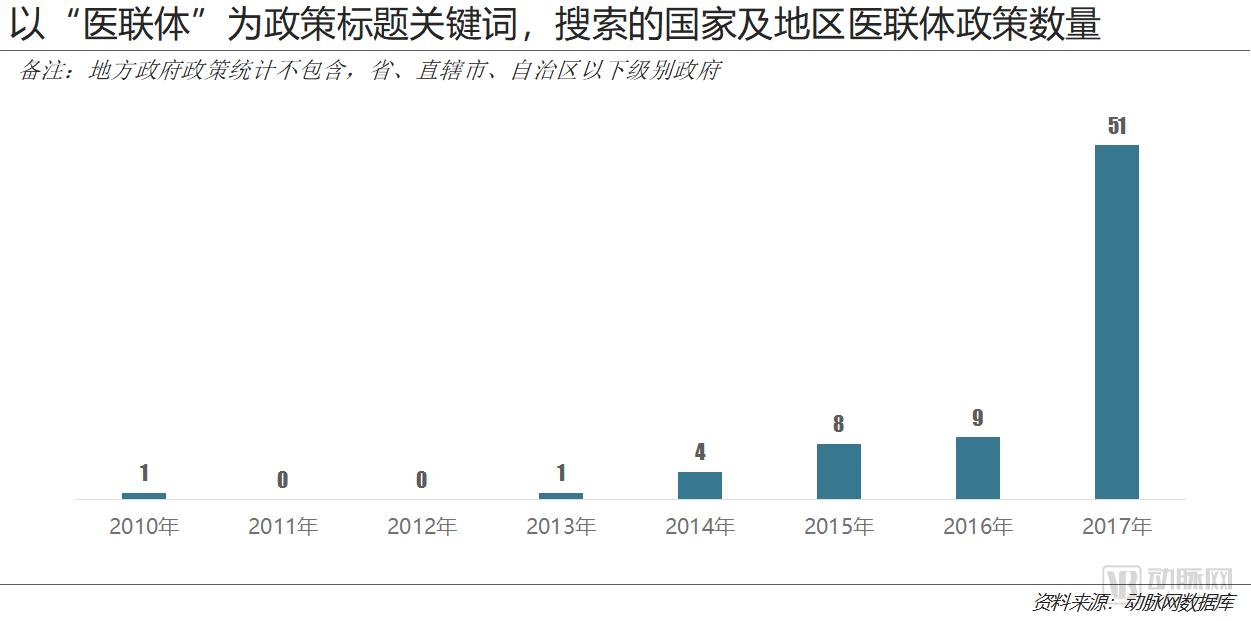
Following the promulgation of the “Guiding Opinions on Strengthening the Construction and Development of Medical Consortia,” there has been a surge in the number of medical consortium-related policies, with every province, municipality directly under the central government, and autonomous region issuing documents in response to the State Council’s policy. In fact, the comprehensive rollout of local policy documents is the primary driver behind the sharp increase in the total number of medical consortium policies.

We have compiled the latest policies related to “Medical Consortiums” in certain regions and identified three key characteristics:
1. Following the release of the State Council’s guiding document on medical consortiums, local governments across China issued regional implementation guidelines for medical consortium development in response. The majority of these policies were introduced in July 2017, indicating that comprehensive promotion of medical consortium construction began nationwide after July 2017.
2. The guidance on the development of medical consortia in various regions aligns with the objectives set by national policies, primarily reflected in the substantial similarity of local development goals for medical consortia. For instance, provisions such as “by 2017, all tertiary hospitals shall participate in the establishment of medical consortia; by 2020, all public secondary hospitals and primary healthcare institutions” are ubiquitous. The construction of medical consortia by governments at all levels has achieved uniformity in approaches and objectives across both horizontal and vertical dimensions, resulting in a largely homogeneous policy environment.
3. The latest policies on medical consortiums in most provinces were issued in July, in response to the national guidelines for the development of medical consortiums. Since then, no new policies have been released, nor have there been any significant changes in policy content. This suggests that a shift in policy direction is unlikely in the future.
It is evident that, driven by local policy responses, the development of Medical Consortia in China has been vigorously rolled out nationwide. Currently, updates to local policies have been relatively slow, and the local implementation of Medical Consortia is proceeding in an orderly manner without significant directional shifts. Consequently, enterprises engaged in the construction of Medical Consortia face low operational risks stemming from policy changes, given the stable policy environment. The establishment of Medical Consortia has essentially become the primary direction for healthcare institution reform. Enterprises can therefore deeply explore policy opportunities without excessive concern about policy-related risks.
3. With over 5,000 entities, medical consortiums deliver tangible operational efficacy
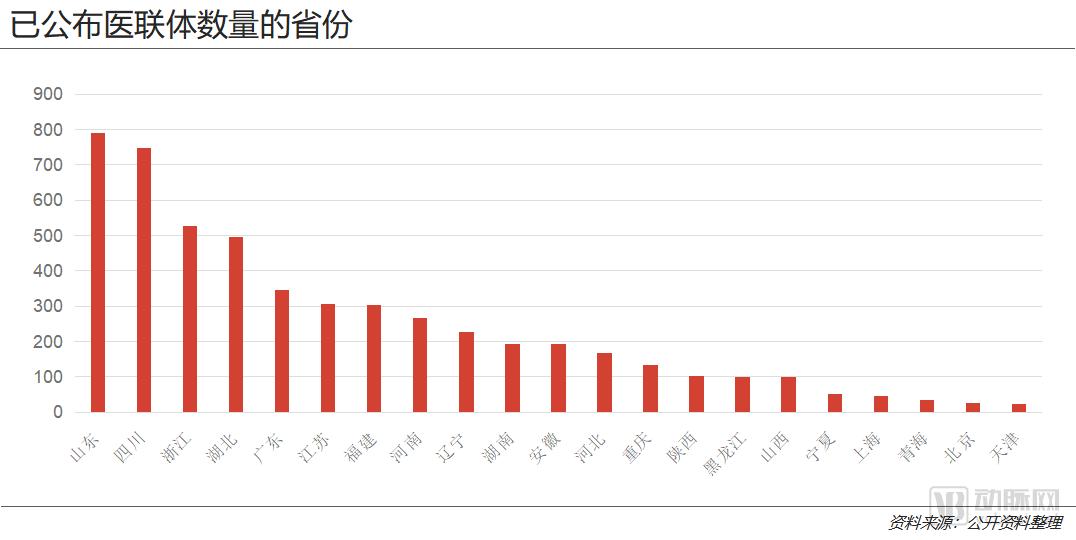
VCBeat Institute has compiled the number of medical consortia in 21 provinces across China based on publicly available information from regional government websites. We have found that there are significant disparities in the number of medical consortia among different provinces. According to the latest figures released by each province, Shandong and Sichuan have the highest numbers, with 790 (as of May 2018) and 747 (as of January 2018) medical consortia, respectively. In contrast, five municipalities and autonomous regions—Tianjin, Beijing, Qinghai, Shanghai, and Ningxia—each have fewer than 50 medical consortia.
There are two reasons for the significant disparities in the number of medical consortia across provinces, municipalities directly under the Central Government, and autonomous regions:
First, although the State Council’s document marked the beginning of the comprehensive establishment of medical consortia, the timing of their implementation varied across provinces. For instance, Shandong, as a pilot province for tiered diagnosis and treatment, had already established more than 700 medical consortia province-wide by July 2017.
Furthermore, the number of healthcare institutions in various regions, particularly tertiary hospitals, can significantly influence the number of medical consortiums.
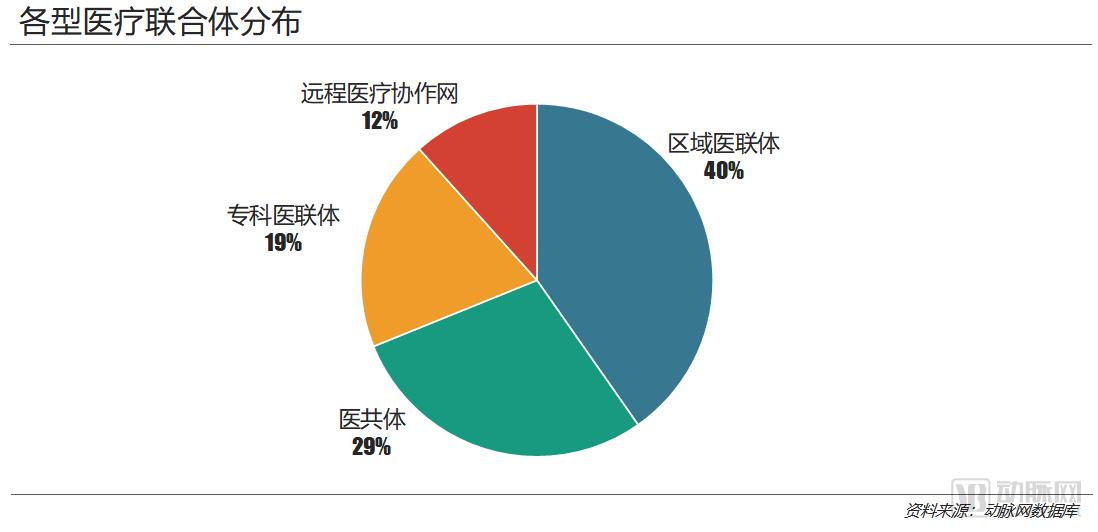
Among the various types of medical consortia, regional medical consortia (i.e., urban medical groups) are the most numerous, accounting for 40% of the total.
The number of telemedicine collaboration networks and specialized medical consortiums is the lowest. This is primarily because telemedicine collaboration networks and specialized alliances are loose-form medical consortiums; such entities have strong coverage capabilities for healthcare institutions, with a single consortium able to encompass numerous facilities, thereby resulting in fewer overall numbers. In contrast, county-level medical communities are tight-knit medical consortiums that face significant challenges in implementation and construction, hence their number is lower than that of regional medical consortiums.
In terms of quantity, China has achieved certain accomplishments in the development of medical consortia; however, whether these consortia have delivered efficiency gains to their member institutions warrants further exploration.

We have collected numerous case studies on the operation of medical consortiums, which demonstrate that:
For tertiary hospitals, referring patients in the rehabilitation phase or those with chronic diseases to lower-tier hospitals can effectively reduce the occupation of medical resources. On one hand, this alleviates hospital congestion and improves the patient experience; on the other hand, it allows medical resources to be allocated to higher-value areas. Furthermore, when lower-tier hospitals actively refer patients they cannot manage, it reduces the diagnostic and treatment burden on tertiary hospitals while improving the quality of their patient pool, ensuring better alignment between patient needs and the hospital’s service capabilities.
For instance, the specialized medical consortium established by Beijing Children’s Hospital attracted a large influx of patients due to its professional influence. In 2014, the hospital’s outpatient volume reached 3.37 million, severely exceeding its service capacity. However, following the establishment of the specialized medical consortium, the outpatient volume decreased by approximately 200,000 in 2015. This effectively alleviated hospital congestion and significantly improved both resource utilization and the patient healthcare experience.
For lower-tier hospitals, the most obvious benefit of patient referrals from higher-tier hospitals is an increase in revenue and operational efficiency. Meanwhile, remote consultations and on-site assistance provided by higher-tier hospitals can significantly enhance the patient capacity of these institutions, enabling them to diagnose and treat patients who were previously beyond their scope of care.
Taking Dejiang County’s “Medical Consortium” as an example, in 2017, outpatient and emergency visits at primary healthcare institutions reached 523,900, representing a year-on-year increase of 25.51% from 417,403 visits in the same period of the previous year, with patient satisfaction reaching 100%. The utilization rate of resources at primary healthcare institutions increased significantly, and revenue levels rose substantially.

4. Six Dimensions: Analyzing Differences Among Various Types of Medical Consortia

Tight-knit medical alliances are primarily established on the basis of ownership and asset integration, implementing unified management of personnel, finances, and materials. Within these organizations, medical institutions at all levels form a genuine community of shared interests and responsibilities. A typical representative is the Tianchang Medical Community in Anhui Province. Generally speaking, medical communities are tight-knit medical alliances.
Hybrid Medical Consortium is a model that initially operates as a relatively loose alliance and gradually transitions into a tightly integrated partnership, typically beginning with integration in specific areas such as assets before evolving into a close-knit consortium. A typical example is the Healthcare Management Group in Qidong City, Jiangsu Province. Generally, most urban medical consortia adopt this model.
Loose-knit medical alliances are established on the basis of contractual relationships, without disrupting the original ownership structures and asset attributes. They maintain independent management in terms of personnel, finances, and materials. Large hospitals provide technical and expert support to lower-tier hospitals, facilitating mutual recognition of information and patient referrals within the alliance. A typical example is the medical alliance in Qingzhou City, Shandong Province. Generally speaking, specialized medical alliances and telemedicine collaboration networks both fall under the category of loose-knit medical alliances.
To examine the specific differences among various medical consortiums, we can uncover their distinct characteristics by analyzing six dimensions: management models, division of responsibilities, human resources management, technical support, resource sharing, and health insurance payment mechanisms.
Management Model:From loose to hybrid and then to tight integration, management models are gradually moving toward unification. Within the Qingzhou Medical Consortium in Shandong (loose type), member institutions maintain their original administrative affiliations and legal entity status, operating with independent accounting. The Qidong Healthcare Management Group in Jiangsu (hybrid type) allows its member units to operate independently with separate accounting under a unified management framework, implementing “five unifications” for integrated management: unified planning, human resources, finance, resource allocation, and performance evaluation. In the Tianchang Medical Community in Anhui (tight type), personnel, finances, and materials are managed and allocated centrally, transforming medical institutions within the consortium into a community of shared development, responsibility, interests, and services.
Responsibilities and Division of Labor:All three types of medical consortia implement a standardized care delivery model featuring initial diagnosis at primary care facilities and two-way referrals. They all mandate that lead hospitals provide targeted assistance and necessary technical support to primary healthcare institutions within the consortium. Among these, tightly integrated medical consortia place greater emphasis on the continuity of care. Taking the Tianchang Medical Community in Anhui Province as an example, while lead hospitals help primary hospitals enhance their capabilities, they also rely on primary hospitals to manage the follow-up phase of patient treatment. Specifically, after discharge, primary healthcare institutions are responsible for ensuring patients adhere to medication schedules and maintain proper diets to prevent relapse and readmission, thereby effectively assuming responsibility for patients referred down from lead hospitals.
Personnel Management:Tight-knit and hybrid medical consortia implement unified management and allocation, making appropriate personnel transfers based on the needs of each institution while keeping the original personnel staffing largely unchanged. In contrast, member institutions within loose-knit medical consortia maintain independent personnel management systems. Among these, both tight-knit and loose-knit medical consortia rely on multi-site practice to facilitate the downward flow of high-quality talent resources. Medical management groups (hybrid type) actively leverage the advantages of corporate management by implementing centralized personnel management and flexible talent mobility.
Technical Support:Medical consortia primarily conduct various technical support activities through institution-to-institution, department-to-department, and individual-to-individual collaborations. For instance, the Jiangsu Qidong Medical Management Group (a hybrid model) explicitly mandates that leading hospitals establish long-term, stable mechanisms for paired assistance, counterpart support, technology sharing, and homogeneous management with subordinate hospitals; that primary departments of leading hospitals partner with primary-level hospitals; and that primary-level hospitals support village clinics. All three types of medical consortia stipulate that leading hospitals regularly dispatch core physicians or specialized teams (such as health management teams, public health service expert guidance groups, and “3+2” general practitioner service teams) to grassroots levels to carry out activities including teaching rounds, outpatient consultations, case consultations, and free clinics. They also encourage qualified physicians to practice at multiple sites in grassroots settings. Notably, the Anhui Tianchang Medical Community (a close-knit model) further requires that qualified medical personnel from leading hospitals establish mentor-mentee relationships with grassroots medical staff to provide more targeted assistance.
Resource Sharing:All three types of medical consortia prioritize the sharing and mutual assistance of internal technical resources, as well as the mutual recognition of test results, with a focus on building various resource-sharing platforms. For instance, the Tianchang (close-knit) model in Anhui Province has established shared centers for laboratory testing, medical imaging, and pathology within the consortium, implementing unified management of large-scale medical equipment for joint use by all member institutions. The Qidong (hybrid) Medical Management Group in Jiangsu Province incorporates more features of corporate management, placing particular emphasis on the establishment of an accounting center. The Qingzhou (loose) medical consortium in Shandong Province focuses more on conducting remote consultations and implements a "universal record" system for outpatient and emergency medical records, as well as a "universal report" system for laboratory and diagnostic test results.
Medical Insurance Payment:As a powerful economic lever, healthcare payment methods play a positive role in aligning the interests of members within medical consortia and promoting orderly patient care-seeking behavior. On the demand side, all three models adopt adjusted deductibles and co-payment ratios, implementing differentiated payment policies to facilitate the orderly flow of patients. On the supply side, the Tianchang Medical Community (close-knit type) in Anhui Province established the Tianchang City Healthcare Security Fund Management Center, consolidating the management of three healthcare security schemes under one center. Payments are made based on a global budget per enrolled individual, with surplus funds distributed among the lead hospital, township health centers, and village clinics in a 6:3:1 ratio. This arrangement fosters a genuine community of shared interests among institutions at all levels within the medical consortium. By transforming patient treatment costs directly into hospital operational costs, this payment reform effectively curbs over-treatment.
5. Management Issues Are the Greatest Obstacle to the Implementation of Medical Consortiums; Currently, the Service Capacity of Primary Healthcare Institutions Is Not the Main Factor Affecting Their Implementation
After integrating into the medical consortium, primary healthcare institutions and tertiary hospitals adopt a model of mutual assistance, establishing mechanisms for collaborative development in diagnostic and treatment technologies, medical equipment, discipline construction, and talent cultivation. This approach implements the operational logic of managing severe cases in hospitals while ensuring that initial consultations take place at the primary care level.
We believe that two-way referral is a key feature of the implementation of medical consortiums in public primary healthcare institutions. Therefore, survey results from physicians and patients regarding “two-way referral” can largely reflect whether the operational logic of medical consortiums has been effectively implemented at the primary care level.
According to a recent survey report published in the Chinese Journal of Health Quality, medical consortium policies have begun to impact public primary healthcare institutions, as most medical institutions have established specific procedures for two-way referrals.
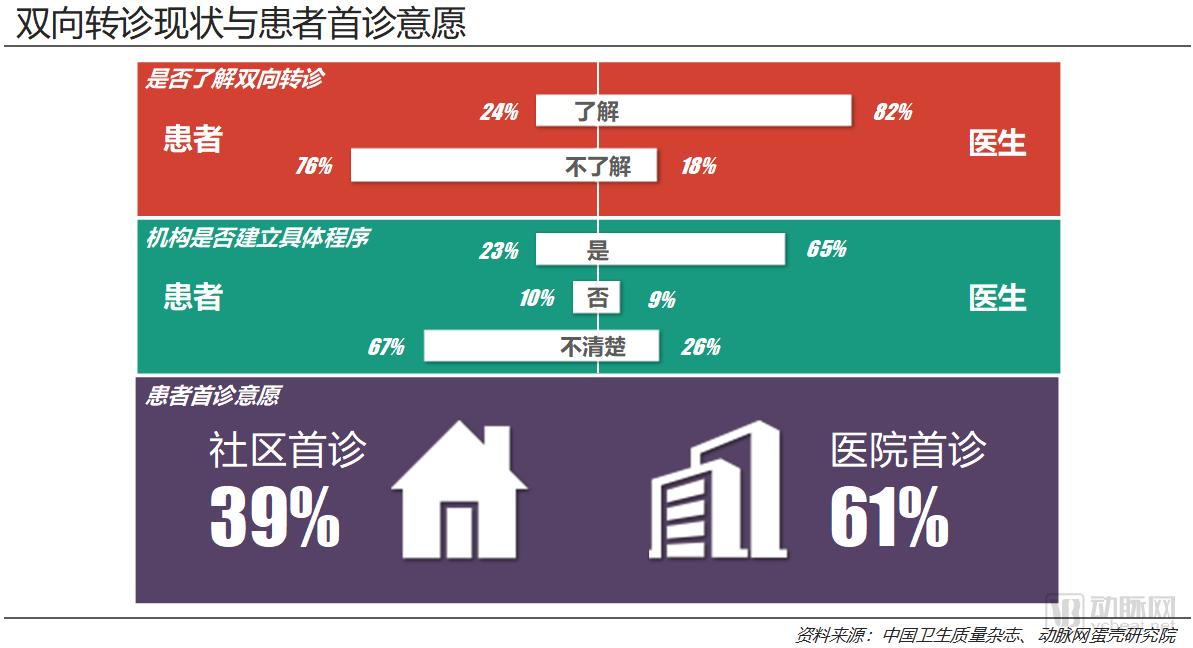
In response to questions about their awareness of the two-way referral system, 82% of physicians reported familiarity with the policy, whereas only 24% of patients indicated similar awareness. Regarding whether healthcare institutions had established specific procedures, 65% of physicians stated that relevant protocols were already in place, with only 26% selecting “unaware.” In stark contrast, patient responses showed an entirely opposite pattern. These two questions yielded completely inverted survey results between physicians and patients. On one hand, this suggests that the framework for two-way referrals has been implemented in most primary healthcare institutions. On the other hand, many patients remain uninformed about this development or even unclear about what two-way referrals entail, indicating that the impact of medical consortia on primary care institutions and the transformation of healthcare access points is still in its early stages. Due to insufficient awareness, patients’ subjective initiative has yet to be fully realized.
However, the survey results still reveal that despite patients’ limited awareness of tiered diagnosis and treatment, two-fifths of them remain willing to seek initial consultation at primary care institutions. Undoubtedly, while primary healthcare facilities have certain shortcomings, they continue to play a significantly important role for patients.
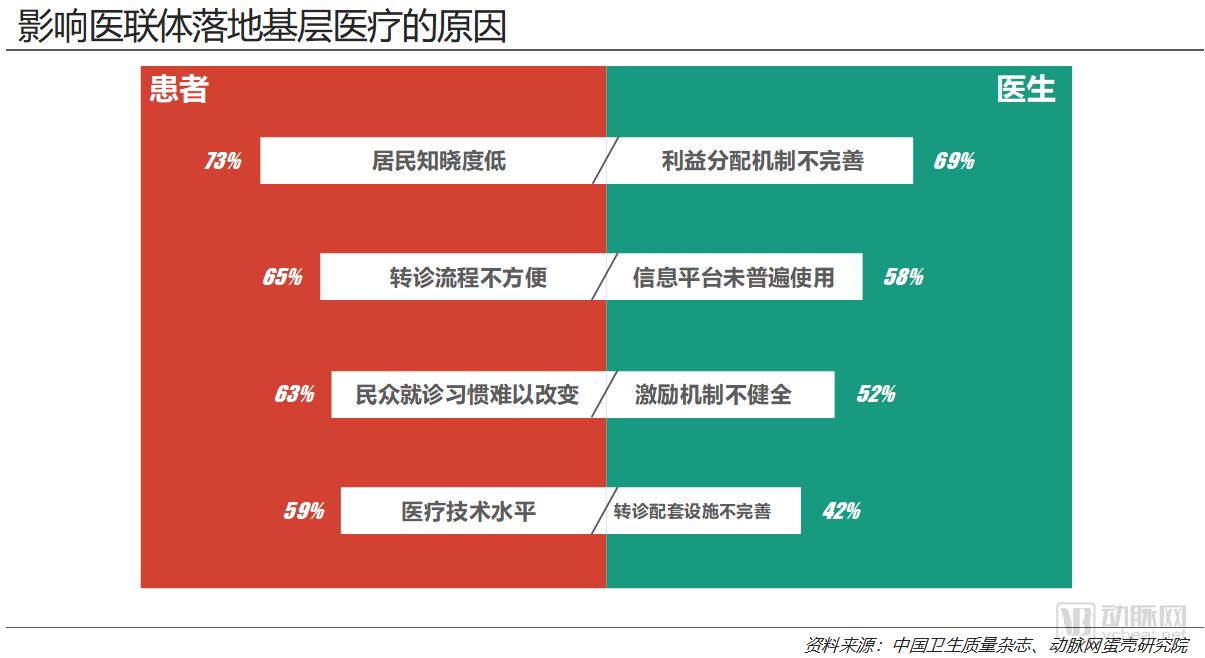
From the patients’ perspective, “low public awareness” is currently the primary factor hindering the implementation of medical consortia at the primary care level. Optimizing referral processes and cultivating consistent healthcare-seeking habits are also critical measures to ensure the successful operation of medical consortia in primary care settings. The option selected by the fewest respondents was “medical technical proficiency,” yet it was still chosen by 59% of patients. This indicates that only after patient education has been strengthened and referral processes optimized will the quality of medical care at the primary level become a major consideration for patients when choosing primary care institutions for their initial consultations.
From physicians’ perspective, management issues within medical consortia are key factors affecting their implementation at the grassroots level. For instance, 69% of physicians selected “imperfect benefit distribution mechanisms,” and 52% chose “inadequate incentive mechanisms.” In addition, infrastructure—such as information platforms and supporting facilities for patient referrals—is also a critical factor influencing the deployment of medical consortia in primary care settings.
The above content is an excerpt from “Reconstructing Healthcare Production Relations to Unlock New Business Opportunities: A Report on the Commercial Value of Medical Consortia.” To read the full report, please follow the VCBeat WeChat official account (vcbeat) or scan the QR code below for direct access.
