For up to $630M, AstraZeneca acquires remaining China rights to AbelZeta’s CAR-T asset

AbelZeta Pharma
Clinical-stage biopharmaceutical company

AbelZeta
Developer of Immune Cell and Stem Cell Therapy Products

AstraZeneca
Biopharmaceutical Manufacturer
On January 16, AbelZeta Pharma announced that AstraZeneca will acquire the remaining China rights to the GPC3 armored CAR-T therapy. Specifically, AstraZeneca will acquire AbelZeta's 50% share of the development and commercialization rights to C-CAR031 in China.
Under the terms of the agreement, AbelZeta will be entitled to receive up to $630 million from AstraZeneca, including an upfront payment and development, regulatory, and sales milestone payments for the GPC3 program in China. Pursuant to a prior agreement, AbelZeta remains eligible to receive additional milestone payments and royalties for development in the rest of world.
As a result, AstraZeneca will acquire the sole right to develop, manufacture, and commercialize C-CAR031 globally. In December 2023, AbelZeta entered into a joint development agreement with AstraZeneca for the co-development and commercialization of C-CAR031 in China.
1Derived from AstraZeneca's Platform Design
C-CAR031 is an autologous, Glypican-3 (GPC3)-targeting chimeric antigen receptor T-cell (CAR-T) therapy. Based on AstraZeneca's novel GPC3-targeting CAR-T candidate (AZD5851), it is designed using AstraZeneca's dominant negative transforming growth factor-beta receptor II (dnTGFβRII) armoring platform and is manufactured by AbelZeta in China. It is currently being investigated for the treatment of hepatocellular carcinoma (HCC) and other solid tumors.
Liver cancer is the third leading cause of cancer death and the sixth most commonly diagnosed cancer worldwide. Categorized based on the originating cell type, hepatocellular carcinoma (HCC) is the most common form of liver cancer—accounting for approximately 75% of primary liver cancers in adults. HCC is one of the most common cancers and a leading cause of cancer-related deaths in China, with approximately 466,000 new cases annually, representing about 50% of global new cases. Roughly 45% of global HCC deaths occur in Greater China.
HCC begins in the liver as either a single tumor or several small nodules. At this local stage, it can be treated with locally targeted or surgical methods. However, most patients are diagnosed at an advanced stage, or their disease progresses to advanced HCC with poor prognosis, resulting in a 5-year survival rate of only 7% and a median survival of approximately 20 months.
GPC3 is a glycoprotein located on the cell surface. It is highly expressed during embryonic development and is overexpressed in a variety of cancers such as HCC and kidney cancer, while showing little to no expression in normal tissues like the liver. This profile gives it dual value as both "tumor-specific" and "functional."
At the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, AbelZeta presented preliminary safety and efficacy results from the first-in-human investigator-initiated trial (IIT) of C-CAR031 in an oral presentation. The report indicated manageable safety and encouraging anti-tumor activity in heavily pretreated patients with advanced HCC who had received 1 to 6 prior lines of therapy.
At a median follow-up of 9.03 months, across all dose levels (DLs), a disease control rate (DCR) of 91.3% and an objective response rate (ORR) of 56.5% were achieved. At DL4, the ORR was 75.0%.
The Phase 1 clinical study, currently ongoing in China, is designed to evaluate the safety and anti-tumor activity of C-CAR031 injection in patients with unresectable HCC. As of March 14, 2024, a total of 24 patients received C-CAR031 infusion across four dose levels (DL). 83.3% (20/24) of patients had extrahepatic metastatic lesions, and the median number of prior lines of therapy was 3.5 (range: 1–6).
Study data showed that as of March 14, 2024, 23 of the 24 enrolled patients were evaluable for efficacy. Tumor reduction was observed in 91.3% of patients, including in both intrahepatic and extrahepatic lesions, with a median reduction of 42.2% (range: -28.1% to 94.4%). The DCR was 91.3%, and the ORR was 56.5% across all DLs. At DL4, the ORR was 75.0%. At a median follow-up of 9.03 months, the Kaplan-Meier estimated median overall survival (mOS) was 11.14 months.
Furthermore, no dose-limiting toxicities or immune effector cell-associated neurotoxicity syndrome (ICANS) were observed in the study. Cytokine release syndrome (CRS) was observed in 22 (91.7%) patients, with the majority (87.5%) being Grade 1/2 CRS. Only one patient (4.2%) experienced Grade 3 CRS.
2Two-Phase Transaction Model to Build CAR-T Clinical Validation in China and Global Ecosystem
As one of the earliest Chinese biopharmaceutical innovators listed on Nasdaq, AbelZeta announced the initiation of its privatization process in late 2019. In February 2021, AbelZeta successfully completed its privatization and delisted from U.S. stock exchanges. In September 2021, AbelZeta completed its post-privatization Series A financing, raising a total of $120 million. This round was co-led by the AstraZeneca CCIC Healthcare Industrial Fund (an existing investor), HSG (formerly known as Sequoia Capital China), and YF Capital, with participation from other existing investors including GIC and TF Capital.
With its two R&D centers in Gaithersburg, Maryland, USA, and Shanghai, China, AbelZeta has established a diversified strategy for the global development of novel drugs. In the United States, the company will leverage its in-house R&D and manufacturing capabilities to establish dynamic partnerships with global pharmaceutical companies to drive the worldwide development of new drug candidates. In China, AbelZeta will utilize its network of Key Opinion Leaders (KOLs) and hospitals to conduct Investigator-Initiated Trials (IITs), enabling early validation of innovative programs and advancing their development within China.
Furthermore, AbelZeta has developed a distinctive two-phase transaction model. The first phase involves granting exclusive rights for development outside of China, combined with a right of first negotiation/co-development option for China. The second phase of collaboration then focuses on selecting competitive indications for the Chinese market and conducting out-licensing based on clinical results generated in China.
In the field of solid tumors, in addition to the recently transacted C-CAR031, AbelZeta is also collaborating with AstraZeneca on the co-development of A-CAR032, a STEAP2-targeting therapy.

AbelZeta Solid Tumor Layout
In the field of hematological malignancies, AbelZeta announced in May 2023 a global exclusive collaboration with Johnson & Johnson Innovative Medicine. The agreement granted exclusive development rights for two CAR-T products, C-CAR039 (Prizloncabtagene autoleucel, a novel bispecific CAR-T targeting CD19/CD20) and C-CAR066 (a novel CD20-targeting CAR-T), outside of China, along with an option right for their development in China. This transaction included an upfront payment of $245 million and potential milestone payments. In December 2023, Johnson & Johnson Innovative Medicine acquired the commercialization rights for these two products in China.
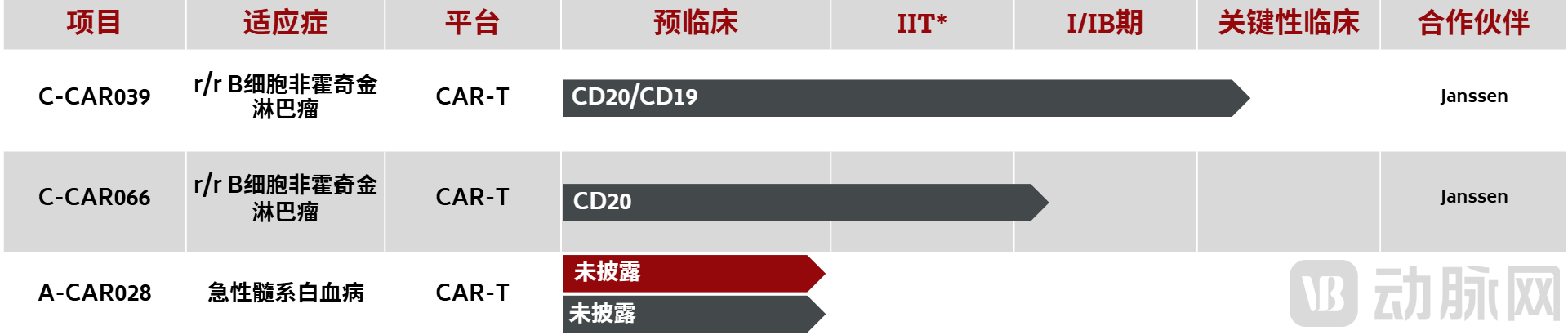
AbelZeta Hematological Tumor Layout
Four-year clinical follow-up results presented at the 2025 European Hematology Association (EHA) Annual Meeting showed that among 48 patients with relapsed or refractory B-cell non-Hodgkin lymphoma (R/R B-NHL) treated with C-CAR039, the overall response rate (ORR) and complete response (CR) rate for all patients were 91.5% and 85.1%, respectively. Among the 43 patients with large B-cell lymphoma (LBCL), the ORR and CR rates were 90.7% and 86.0%, respectively. With a median follow-up of 45.5 months (range: 3.1–62.8 months), the median duration of response (DOR), progression-free survival (PFS), and overall survival (OS) were not reached for all patients.
According to data presented at the 65th American Society of Hematology (ASH) Annual Meeting, a study of C-CAR066 for the treatment of r/r LBCL in patients who had failed prior CD19 CAR-T therapy showed that, with a median follow-up of 27.7 months, the ORR was 92.9% and the CR rate was 57.1%.
Deepening its roots in China and leveraging China's clinical resources and manufacturing advantages to build a global biopharmaceutical ecosystem is the core strategy for AbelZeta.
On the manufacturing front, AbelZeta operates GMP-compliant facilities in Shanghai, Beijing, and Wuxi, China, meeting both FDA and Chinese national standards. The total area exceeds 3,000 square meters, featuring 12 independent production lines. It is also one of the few cell therapy technology companies in China certified by the international SGS to comply with the ISO9001 quality management system. The company possesses clinical-grade, standardized cell preparation processes and supporting technologies, with over a thousand Standard Management Procedures (SMPs) and Standard Operating Procedures (SOPs).
Earlier information indicates that AbelZeta maintains cell banks in multiple cities capable of storing over 200,000 donor-derived cell samples. It also operates a state-of-the-art cold-chain temperature control system (IT cloud-based system) for monitoring cell culture, storage, and transportation. The Shanghai facility includes a "Joint Cell Therapy Laboratory" established with GE Healthcare and a "Joint Cell Therapy Technology Innovation and Application Center" in collaboration with Thermo Fisher.
In late September 2018, Novartis and AbelZeta entered into a collaboration for the manufacturing of Kymriah in China. AbelZeta was primarily responsible for the manufacturing process, while Novartis was responsible for distribution, regulatory affairs, and commercialization in China. Under the agreement, AbelZeta sold approximately 9% of its equity to Novartis at $27.43 per share, receiving an equity purchase payment of $40 million. Novartis gained certain royalty-free intellectual property rights related to specific CAR-T technologies from AbelZeta globally. AbelZeta received single-digit tiered collaboration payments based on net product sales and a markup on manufacturing costs from Novartis.
Currently, AbelZeta's pipeline comprises over ten investigational products spanning hematological tumors, autoimmune diseases, and solid tumors. It also possesses next-generation cell therapies for solid tumors (including armored CAR-T and Tumor-Infiltrating Lymphocyte (TIL) therapies), such as the novel autologous BCMA-targeting CAR-T product C-CAR088, the solid tumor TIL product C-TIL051, a stem cell exosome therapy, among others. AbelZeta is also accelerating the clinical and commercialization process for AlloJoin®, its allogeneic adipose-derived mesenchymal stem cell therapy for knee osteoarthritis, which is in the late stages of Phase 2 clinical development.
In 2023, its allogeneic human adipose-derived mesenchymal progenitor cell injection, AlloJoin, initiated Phase 3 clinical trials. In 2025, AbelZeta updated the clinical protocol with the Center for Drug Evaluation (CDE), setting dual primary endpoints for the Phase 3 trial based on WOMAC score and knee joint cavity structural improvement. This marks the first time joint structure and functional improvement have been introduced as one of the two main evaluation criteria.

AbelZeta Inflammation and Immune Disease Layout